🧠 CHAPTER 8 — URINARY SYSTEM
⚙ 1. ANATOMY AND FUNCTION OVERVIEW
Components:
Kidneys (2) – retroperitoneal, T12–L3 level; right lower than left.
Ureters (2) – carry urine to bladder.
Urinary bladder – stores urine. Urethra – excretes urine.
Functions:
Excretion of metabolic wastes (urea, creatinine, uric acid).
Regulation of water, electrolytes, and pH.
Endocrine functions: Renin (BP control), Erythropoietin (RBC production),
Vitamin D activation.
Microscopic unit: Nephron — glomerulus + tubules; filters ~180 L/day.
🩻 2. IMAGING MODALITIES AND THEIR ROLES
Modality Role / Findings
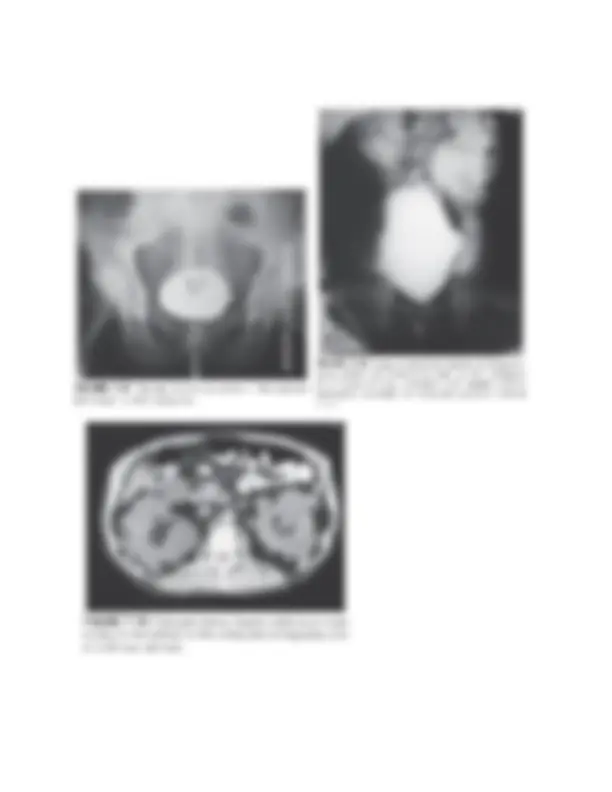
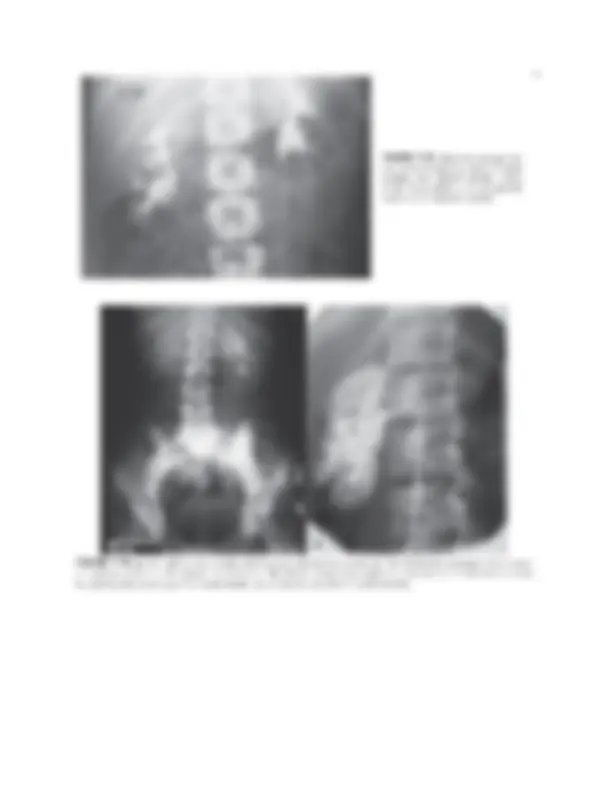
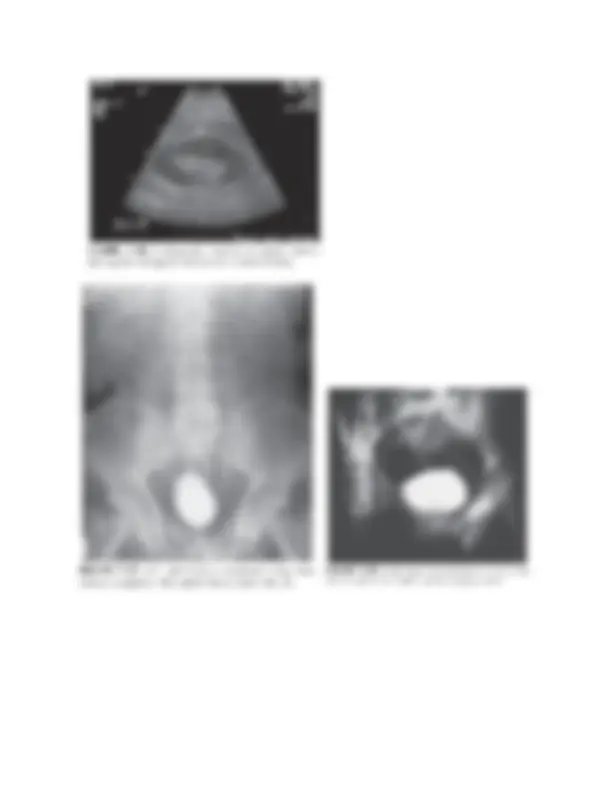
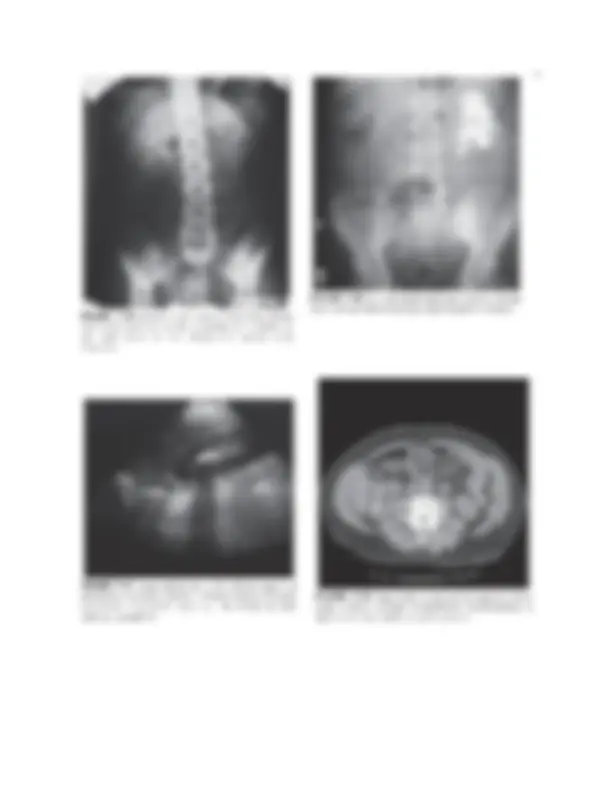
Radiography (KUB) Demonstrates calcifications, renal size, position.
Intravenous urography (IVU/IVP) Shows collecting system anatomy and function
(now less common).
Sonography First-line for hydronephrosis, cysts, masses,
bladder volume, obstruction; no radiation.
CT (with/without contrast) Gold standard for renal/ureteric stones, trauma,
staging of tumors.
MRI Characterizes masses, evaluates renal veins and
IVC involvement; MR urography for function.
Nuclear Medicine (DMSA, MAG-3
scans) Renal perfusion and differential function.