Download chapter seven notes c and more Study notes Anatomy in PDF only on Docsity!
234
CHAPTER 8
As noted in Chapter 7, the two main divisions of the skeletal system are the axial skeleton and the appendicular skeleton. As you learned in that chapter, the general function of the axial skeleton is the protection of internal organs; the primary function of the appendicular skeleton, the focus of this chapter, is movement. The appendicular skeleton includes the bones that make up the upper and lower limbs as well as the bones
of the two girdles that attach the limbs to the axial skeleton. The bones of the appendicular skeleton are connected with one another and with skeletal muscles, permitting you to do things such as walk, write, use a computer, dance, swim, and play a musical instrument.
Q Did you ever wonder what causes runner’s knee?
The Skeletal System:
The Appendicular Skeleton
The Appendicular Skeleton and Homeostasis
The bones of the appendicular skeleton contribute to homeostasis by providing attachment points and leverage for muscles, which aids body movements; by providing support and protection of internal organs, such as the reproductive organs; and by storing and releasing calcium.
8.1 Pectoral (Shoulder) Girdle 235
8.1 Pectoral (Shoulder) Girdle
OBJECTIVE
- Identify the bones of the pectoral (shoulder) girdle, their functions, and their principal markings.
The human body has two pectoral (shoulder) girdles (PEK-tō-ral) that attach the bones of the upper limbs to the axial skeleton ( Figure 8.1 ). Each of the two pectoral girdles consists of a clavicle and a scapula.
The clavicle is the anterior bone and articulates with the manubrium of the sternum at the sternoclavicular joint. The scapula articulates with the clavicle at the acromioclavicular joint and with the humerus at the glenohumeral (shoulder) joint. The pectoral girdles do not artic- ulate with the vertebral column and are held in position and stabilized by a group of large muscles that extend from the vertebral column and ribs to the scapula.
Clavicle
Each slender, S -shaped clavicle (KLAV-i-kul = key), or collarbone, lies horizontally across the anterior part of the thorax superior to
Scapula
Pectoral girdle: Clavicle
Acromioclavicular joint
Glenohumeral joint
Clavicle
Clavicle
Scapula
Scapula
Vertebrae
Rib
Sternum
Sternoclavicular joint
Rib
Humerus
(a) Anterior view of pectoral girdle (b) Posterior view of pectoral girdle
Humerus
FIGURE 8.1 Right pectoral (shoulder) girdle.
The clavicle is the anterior bone of the pectoral girdle, and the scapula is the posterior bone.
Q What is the function of the pectoral girdle?
8.1 Pectoral (Shoulder) Girdle 237
the shoulder. Tailors measure the length of the upper limb from the acromion. As noted earlier, the acromion articulates with the acromial end of the clavicle to form the acromioclavicular joint. Inferior to the acromion is a shallow depression, the glenoid cavity, that accepts the head of the humerus (arm bone) to form the glenohumeral (shoulder) joint (see Figure 8.1 ). The thin edge of the scapula closer to the vertebral column is called the medial (vertebral) border. The thick edge of the scapula closer to the arm is called the lateral (axillary) border. The medial and lateral borders join at the inferior angle. The superior edge of the scapula, called the superior border, joins the medial border at the superior angle. The scapular notch is a prominent indentation along the superior border through which the suprascapular nerve passes. At the lateral end of the superior border of the scapula is a projec- tion of the anterior surface called the coracoid process (KOR-a-koyd = like a crow’s beak), to which the tendons of muscles (pectoralis minor, coracobrachialis, and biceps brachii) and ligaments (coracoacromial, conoid, and trapezoid) attach. Superior and inferior to the spine on
the posterior surface of the scapula are two fossae: The supraspinous fossa (sū-pra-SPĪ-nus) is a surface of attachment for the supraspina- tus muscle of the shoulder, and the infraspinous fossa (in-fra-SPĪ-nus) serves as a surface of attachment for the infraspinatus muscle of the shoulder. On the anterior surface of the scapula is a slightly hollowed- out area called the subscapular fossa, a surface of attachment for the subscapularis muscle.
Checkpoint
1. What is the function of the pectoral girdle? 2. Which joints are formed by the articulation of the clavicle with other bones? Which areas of the clavicle are involved in each joint? 3. Which joints are formed by the scapula with other bones? What are the names of the parts of the scapula that form each joint?
FIGURE 8.3 Right scapula (shoulder blade).
The glenoid cavity of the scapula articulates with the head of the humerus to form the glenohumeral (shoulder) joint.
Scapula
Acromion
Coracoid process Glenoid cavity
Lateral (axillary) border
(a) Anterior view
MEDIAL
Medial (vertebral) border
Inferior angle
Subscapular fossa
Scapular notch
Superior border
Superior angle
Q Which part of the scapula forms the high point of the shoulder?
(b) Posterior view (c) Lateral view
MEDIAL
Acromion Coracoid process
Glenoid cavity
Lateral (axillary) border
Spine
Inferior angle
Medial (vertebral) border
Supraspinous fossa
Infraspinous fossa
Scapular notch
Superior border
Superior angle
238 CHAPTER 8 The Skeletal System: The Appendicular Skeleton
rough projections on either side of the distal end of the humerus to which the tendons of most muscles of the forearm are attached. The ulnar nerve may be palpated by rolling a finger over the skin surface above the posterior surface of the medial epicondyle. This nerve is the one that makes you feel a very severe pain when you hit your elbow, which for some reason is commonly referred to as the funnybone, even though this event is anything but funny.
Skeleton of the Forearm—
Ulna and Radius
The ulna is located on the medial aspect (the little-finger side) of the forearm and is longer than the radius ( Figure 8.5 ). A convenient mne- monic to help you remember the location of the ulna in relation to the hand is “p.u.” (the p inky is on the u lna side). At the proximal end of the ulna ( Figure 8.5b ) is the olecranon, which forms the prominence of the elbow. With the olecranon, an anterior projection called the coronoid process ( Figure 8.5a ) articu- lates with the trochlea of the humerus. The trochlear notch is a large curved area between the olecranon and coronoid process that forms part of the elbow joint (see Figure 8.6b ). Lateral and inferior to the trochlear notch is a depression, the radial notch, which articulates with the head of the radius. Just inferior to the coronoid process is the ulnar tuberosity, to which the biceps brachii muscle attaches. The dis- tal end of the ulna consists of a head that is separated from the wrist by a disc of fibrocartilage. A styloid process is located on the posterior side of the ulna’s distal end. It provides attachment for the ulnar col- lateral ligament to the wrist. The radius is the smaller bone of the forearm and is located on the lateral aspect (thumb side) of the forearm ( Figure 8.5a ). In contrast to the ulna, the radius is narrow at its proximal end and widens at its distal end. The proximal end of the radius has a disc-shaped head that articulates with the capitulum of the humerus and the radial notch of the ulna. Inferior to the head is the constricted neck. A rough- ened area inferior to the neck on the anteromedial side, called the radial tuberosity, is a point of attachment for the tendons of the biceps brachii muscle. The shaft of the radius widens distally to form a styloid process on the lateral side, which can be felt proxi- mal to the thumb. The distal end of the radius contains a narrow concavity, the ulnar notch, which articulates with the head of the ulna. The styloid process provides attachment for the brachioradialis muscle and for attachment of the radial collateral ligament to the wrist. Fracture of the distal end of the radius is the most common fracture in adults older than 50, typically occurring during a fall. The ulna and radius articulate with the humerus at the elbow joint. The articulation occurs in two places ( Figure 8.6a, b ): where the head of the radius articulates with the capitulum of the humerus, and where the trochlear notch of the ulna articulates with the trochlea of the humerus. The ulna and the radius connect with one another at three sites. First, a broad, flat, fibrous connective tissue called the
8.2 Upper Limb (Extremity)
OBJECTIVE
- Identify the bones of the upper limb and their principal markings.
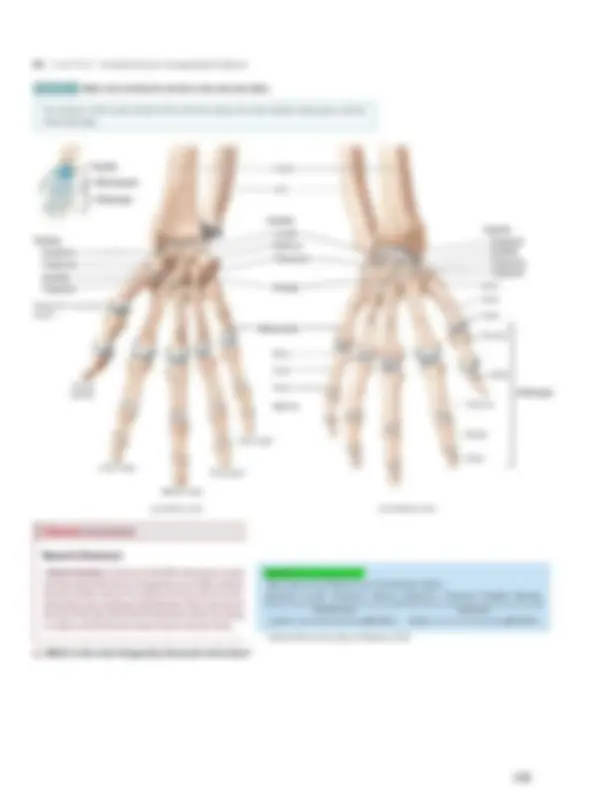
Each upper limb (upper extremity) has 30 bones in three locations— (1) the humerus in the arm; (2) the ulna and radius in the forearm; and (3) the 8 carpals in the carpus (wrist), the 5 metacarpals in the meta- carpus (palm), and the 14 phalanges (bones of the digits) in the hand (see Figures 8.4 and 8.5 ).
Skeleton of the Arm—Humerus
The humerus (HŪ-mer-us), or arm bone, is the longest and largest bone of the upper limb ( Figure 8.4 ). It articulates proximally with the scapula and distally with two bones, the ulna and the radius, to form the elbow joint. The proximal end of the humerus features a rounded head that articulates with the glenoid cavity of the scapula to form the gleno- humeral (shoulder) joint. Distal to the head is the anatomical neck, which is visible as an oblique groove. It is the former site of the epi- physeal (growth) plate in an adult humerus. The greater tubercle is a lateral projection distal to the anatomical neck. It is the most later- ally palpable bony landmark of the shoulder region and is immedi- ately inferior to the palpable acromion of the scapula mentioned earlier. The lesser tubercle projects anteriorly. Between the two tubercles there is a groove named the intertubercular sulcus. The sur- gical neck is a constriction in the humerus just distal to the tubercles, where the head tapers to the shaft; it is so named because fractures often occur here. The body (shaft) of the humerus is roughly cylindrical at its prox- imal end, but it gradually becomes triangular until it is flattened and broad at its distal end. Laterally, at the middle portion of the shaft, there is a roughened, V-shaped area called the deltoid tuberosity. This area serves as a point of attachment for the tendons of the del- toid muscle. On the posterior surface of the humerus is the radial groove, which runs along the deltoid tuberosity and contains the radial nerve. Several prominent features are evident at the distal end of the humerus. The capitulum (ka-PIT-ū-lum; capit- = head) is a rounded knob on the lateral aspect of the bone that articulates with the head of the radius. The radial fossa is an anterior depression above the capitulum that articulates with the head of the radius when the forearm is flexed (bent). The trochlea (TROK-lē-a = pulley), located medial to the capitulum, is a spool-shaped surface that articulates with the trochlear notch of the ulna. The coronoid fossa (KOR-ō- noyd = crown-shaped) is an anterior depression that receives the coronoid process of the ulna when the forearm is flexed. The olec- ranon fossa (ō-LEK-ra-non = elbow) is a large posterior depression that receives the olecranon of the ulna when the forearm is extended (straightened). The medial epicondyle and lateral epicondyle are
240 CHAPTER 8 The Skeletal System: The Appendicular Skeleton
- trapezium (tra-PE- -zē-um = four-sided figure with no two sides parallel)
- trapezoid (TRAP-e-zoyd = four-sided figure with two sides parallel)
- capitate (KAP-i-tāt = head-shaped)
- hamate (HAM-āt = hooked).
- triquetrum (trī-KWE- -trum = three-cornered)
- pisiform (PĪS-i-form = pea-shaped).
The proximal row of carpals articulates with the distal ends of the ulna and radius to form the wrist joint. The carpals in the distal row, from lateral to medial, are the
FIGURE 8.5 Right ulna and radius in relation to the humerus and carpals.
In the forearm, the longer ulna is on the medial side, and the shorter radius is on the lateral side.
Olecranon Head of radius Neck of radius
Radius
Olecranon fossa
Styloid process of radius
MEDIAL
MEDIAL
Ulna
Interosseous membrane
Carpals
Styloid process of ulna
Humerus
Coronoid process
Ulnar tuberosity Radial tuberosity
Trochlea
Coronoid fossa
Head of ulna
Styloid process of radius
Capitulum
Radial fossa
Neck of radius
Head of radius
Radius Ulna
Radius
(a) Anterior view (b) Posterior view
Q What part of the ulna is called the “elbow”?
8.2 Upper Limb (Extremity) 241
FIGURE 8.6 Articulations formed by the ulna and radius. (a) Elbow joint. (b) Joint surfaces at proximal end of the ulna. (c) Joint surfaces at distal ends of radius and ulna.
The elbow joint is formed by two articulations: (1) the trochlear notch of the ulna with the trochlea of the humerus and (2) the head of the radius with the capitulum of the humerus.
(a) Medial view in relation to humerus
Humerus
Radius
Ulna Coronoid process
Radial tuberosity
Interosseous membrane
Head Capitulum Trochlea
Coronoid fossa
Medial epicondyle of humerus
View
Ulna
Radius
Olecranon
Trochlear notch
Coronoid process Radial notch
Ulnar tuberosity
Ulna
(b) Lateral view of proximal end of ulna
Q How many points of attachment are there between the radius and ulna?
Radius Ulna
View
Styloid process
Head
Ulnar notch of radius
Ulna
MEDIAL
Interosseous membrane
Radius
Articulation for scaphoid
Articulation for lunate
Styloid process
(c) Inferior view of distal ends of radius and ulna
The capitate is the largest carpal bone; its rounded projection, the head, articulates with the lunate. The hamate is named for a large hook-shaped projection on its anterior surface. In about 70% of carpal fractures, only the scaphoid is broken. This is because the force of a
fall on an outstretched hand is transmitted from the capitate through the scaphoid to the radius. The anterior concave space formed by the pisiform and hamate (on the ulnar side), and the scaphoid and trapezium (on the radial
8.3 Pelvic (Hip) Girdle 243
the thumb, these other four digits are commonly referred to as the index finger, middle finger, ring finger, and little finger. The proximal phalanges of all digits articulate with the metacarpal bones. The middle phalanges of the fingers (II–V) articulate with their distal phalanges. (The proximal phalanx of the thumb [I] articulates with its distal phalanx.) Joints between phalanges are called interphalan- geal joints.
Checkpoint
4. Name the bones that form the upper limb, from proximal to distal. 5. Distinguish between the anatomical neck and the surgical neck of the humerus. Name the proximal and distal points formed by the humerus, and indicate which parts of the bones are involved. 6. How many joints are formed between the ulna and radius, what are their names, and what parts of the bones are involved? 7. Which is more distal, the base or the head of the meta carpals? With which bones do the proximal phalanges articulate?
8.3 Pelvic (Hip) Girdle
OBJECTIVE
- Identify the bones of the pelvic girdle and their principal markings.
The pelvic (hip) girdle consists of the two hip bones , also called coxal (KOK-sal; cox- = hip) or pelvic bones or os coxa ( Figure 8.8 ). The hip bones unite anteriorly at a joint called the pubic symphysis (PŪ-bik SIM-fi-sis). They unite posteriorly with the sacrum at the
side), with the rooflike covering of the flexor retinaculum (strong fibrous bands of connective tissue) is the carpal tunnel. The long flexor tendons of the digits and thumb and the median nerve pass through the carpal tunnel. Narrowing of the carpal tunnel, due to such factors as inflammation, may give rise to a condition called carpal tunnel syndrome (described in Clinical Connection: Carpal Tunnel Syndrome in Exhibit 11.O ). There is a useful mnemonic for learning the names of the carpal bones provided in Figure 8.7. The first letter of the carpal bones from lateral to medial (proximal row, then distal row) corresponds to the first letter of each word in the mnemonic.
Metacarpals The metacarpus (meta- = beyond), or palm, is the intermediate region of the hand and consists of five bones called metacarpals. Each metacarpal bone consists of a proximal base, an intermedi- ate shaft, and a distal head ( Figure 8.7b ). The metacarpal bones are numbered I to V (or 1–5), starting with the thumb, from lateral to me- dial. The bases articulate with the distal row of carpal bones to form the carpometacarpal joints. The heads articulate with the proximal phalanges to form the metacarpophalangeal joints. The heads of the metacarpals, commonly called “knuckles,” are readily visible in a clenched fist.
Phalanges The phalanges (fa-LAN-jēz; phalan- = a battle
line), or bones of the digits, make up the distal part of the hand. There are 14 phalanges in the five digits of each hand and, like the metacarpals, the digits are numbered I to V (or 1–5), beginning with the thumb, from lateral to medial. A single bone of a digit is referred to as a phalanx (FA- lanks). Each phalanx consists of a proximal base, an intermediate shaft, and a distal head. The thumb (pollex) has two phalanges called proximal and distal phalanges. The other four digits have three pha- langes called proximal, middle, and distal phalanges. In order from
FIGURE 8.8 Bony pelvis. Shown here is the female bony pelvis.
The hip bones unite anteriorly at the pubic symphysis and posteriorly at the sacrum to form the bony pelvis.
Pelvic (hip) girdle Sacroiliac joint Sacral promontory Pelvic brim Acetabulum
Obturator foramen
Hip bone
Sacrum
Coccyx Pubic symphysis
Anterosuperior view of pelvic girdle
Q What are the functions of the bony pelvis?
244 CHAPTER 8 The Skeletal System: The Appendicular Skeleton
FIGURE 8.9 Right hip bone. The lines of fusion of the ilium, ischium, and pubis depicted in part (a) and (b) are not always visible in an adult.
The acetabulum is the socket for the head of the femur, where the three parts of the hip bone converge and ossify.
Ischium
Ilium
Pubis
ANTERIOR
SUPERIOR
(a) Lateral view showing parts of hip bone
Posterior superior iliac spine
Gluteal lines Anterior Inferior Posterior Ilium
Ischium
Pubis
Posterior inferior iliac spine Greater sciatic notch Body of ischium
Ischial spine Lesser sciatic notch Ischial tuberosity
Iliac crest
Ala
Tubercle of the iliac crest
Obturator foramen
Body of ilium
Anterior inferior iliac spine
Anterior superior iliac spine
Inferior ramus of pubis
Acetabulum Acetabular notch
Superior ramus of pubis
Ramus of ischium
Pubic tubercle
ANTERIOR
(b) Detailed lateral view
sacroiliac joints. The complete ring composed of the hip bones, pubic symphysis, sacrum, and coccyx forms a deep, basinlike structure called the bony pelvis (pelv- = basin). The plural is pelves (PEL-vēz) or pelvises. Functionally, the bony pelvis provides a strong and stable support for the vertebral column and pelvic and lower abdominal organs. The pelvic girdle of the bony pelvis also connects the bones of the lower limbs to the axial skeleton. Each of the two hip bones of a newborn consists of three bones separated by cartilage: a superior ilium, an inferior and anterior pubis, and an inferior and posterior ischium. By age 23, the three separate bones fuse together ( Figure 8.9a ). Although the hip bones function as single bones, anatomists commonly discuss each hip bone as three separate bones.
Ilium
The ilium (IL-ē-um = flank), the largest of the three components of the hip bone ( Figure 8.9b ), is composed of a superior ala (= wing) and an inferior body. The body is one of the components of the ace- tabulum, the socket for the head of the femur. The superior border of the ilium, the iliac crest, ends anteriorly in a blunt anterior superior iliac spine. Bruising of the anterior superior iliac spine and associ- ated soft tissues, such as occurs in body contact sports, is called a hip pointer. Below this spine is the anterior inferior iliac spine. Pos- teriorly, the iliac crest ends in a sharp posterior superior iliac spine.
Below this spine is the posterior inferior iliac spine. The spines serve as points of attachment for the tendons of the muscles of the trunk, hip, and thighs. Below the posterior inferior iliac spine is the greater sciatic notch (sī-AT-ik), through which the sciatic nerve (the longest nerve in the body) passes, along with other nerve and muscles. The medial surface of the ilium contains the iliac fossa, a concav- ity where the tendon of the iliacus muscle attaches. Posterior to this fossa are the iliac tuberosity, a point of attachment for the sacroiliac ligament, and the auricular surface (auric- = ear-shaped), which ar- ticulates with the sacrum to form the sacroiliac joint (see Figure 8.8 ). Projecting anteriorly and inferiorly from the auricular surface is a ridge called the arcuate line (AR-kū-āt; arc- = bow). The other conspicuous markings of the ilium are three arched lines on its lateral surface called the posterior gluteal line (glut- = but- tock), the anterior gluteal line, and the inferior gluteal line. The gluteal muscles attach to the ilium between these lines.
Ischium
The ischium (IS-kē-um = hip), the inferior, posterior portion of the hip bone ( Figure 8.9b, c ), comprises a superior body and an inferior ramus (ram- = branch; plural is rami). The ramus is the portion of the ischium that fuses with the pubis. Features of the ischium include the promi- nent ischial spine, a lesser sciatic notch below the spine, and a rough and thickened ischial tuberosity. Because this prominent tuberosity is
246 CHAPTER 8 The Skeletal System: The Appendicular Skeleton
portion of the urinary bladder (when it is full) and the lower intestines in both genders and the uterus, ovaries, and uterine tubes of the female. The portion of the bony pelvis inferior to the pelvic brim is the true (lesser) pelvis ( Figure 8.10b ). It has an inlet, an outlet, and a cavity. It is bounded by the sacrum and coccyx posteriorly, inferior portions of the ilium and ischium laterally, and the pubic bones an- teriorly. The true pelvis surrounds the pelvic cavity, which was de- scribed in Chapter 1 (see Figure 1.9 ). The true pelvis contains the rectum and urinary bladder in both genders, the vagina and cervix of the uterus in females, and the prostate in males. The superior opening of the true pelvis, bordered by the pelvic brim, is called the pelvic inlet; the inferior opening of the true pelvis is the pelvic
by following the landmarks around parts of the hip bones to form the outline of an oblique plane. Beginning posteriorly at the sacral prom- ontory of the sacrum, trace laterally and inferiorly along the arcuate lines of the ilium. Continue inferiorly along the pectineal lines of the pubis. Finally, trace anteriorly along the pubic crest to the superior portion of the pubic symphysis. Together, these points form an oblique plane that is higher in the back than in the front. The circumference of this plane is the pelvic brim. The portion of the bony pelvis superior to the pelvic brim is re- ferred to as the false (greater) pelvis ( Figure 8.10b ). It is bordered by the lumbar vertebrae posteriorly, the upper portions of the hip bones laterally, and the abdominal wall anteriorly. The space enclosed by the false pelvis is part of the lower abdomen; it contains the superior
FIGURE 8.10 True and false pelves. Shown here is the female pelvis. For simplicity, in part (a) the landmarks of the pelvic brim are shown only on the left side of the body, and the outline of the pelvic brim is shown only on the right side. The entire pelvic brim is shown in Table 8..
The true and false pelves are separated by the pelvic brim.
(a) Anterosuperior view of pelvic girdle
Arcuate line
Hip bone
Sacrum
Pelvic brim
Pectineal line Pubic crest
Pubic symphysis
Sacral promontory
Pelvic brim landmarks:
Sacral promontory
False pelvis
Plane of pelvic brim
Pelvic axis
Pubic symphysis
(b) Midsagittal section indicating locations of true (blue) and false (pink) pelves
ANTERIOR
Sacrum
Midsagittal plane
Sacral canal
True pelvis
Coccyx
Plane of pelvic outlet
8.6 Lower Limb (Extremity) 247
(c) Anterosuperior view of false pelvis (pink) (d) Anterosuperior view of true pelvis (blue)
Q What is the significance of the pelvic axis?
outlet, which is covered by the muscle at the floor of the pelvis. The pelvic axis is an imaginary line that curves through the true pelvis from the central point of the plane of the pelvic inlet to the central point of the plane of the pelvic outlet. During childbirth the pelvic axis is the route taken by the baby’s head as it descends through the pelvis.
Clinical Connection
Pelvimetry
Pelvimetry is the measurement of the size of the inlet and outlet of the birth canal, which may be done by ultrasonography or physical examina- tion. Measurement of the pelvic cavity in pregnant females is important because the fetus must pass through the narrower opening of the pelvis at birth. A cesarean section is usually planned if it is determined that the pelvic cavity is too small to permit passage of the baby.
Checkpoint
11. Why are the false and true pelves important clinically?
8.5 Comparison of Female
and Male Pelves
OBJECTIVE
- Compare the principal differences between female and male pelves.
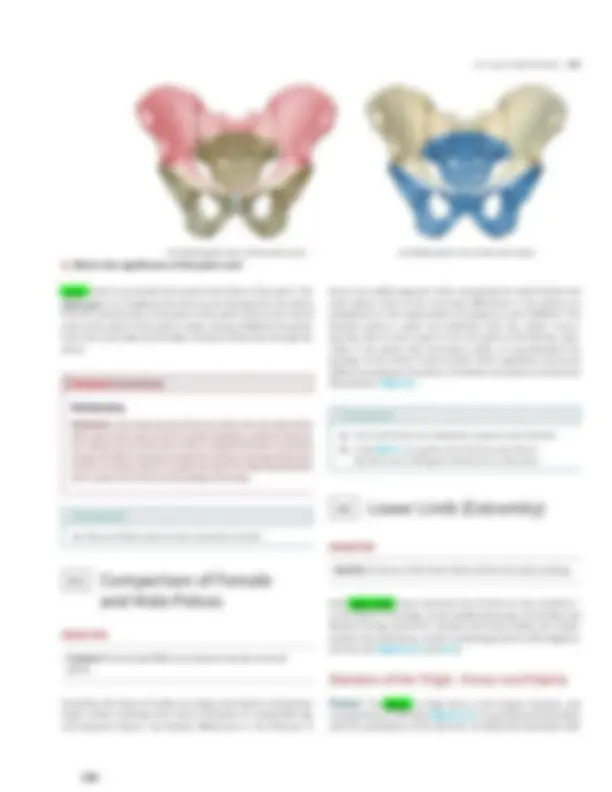
Generally, the bones of males are larger and heavier and possess larger surface markings than those of females of comparable age and physical stature. Sex-related differences in the features of
bones are readily apparent when comparing the adult female and male pelves. Most of the structural differences in the pelves are adaptations to the requirements of pregnancy and childbirth. The female’s pelvis is wider and shallower than the male’s. Conse- quently, there is more space in the true pelvis of the female, espe- cially in the pelvic inlet and pelvic outlet, to accommodate the passage of the infant’s head at birth. Other significant structural differences between the pelves of females and males are listed and illustrated in Table 8..
Checkpoint
12. How is the female pelvis adapted for pregnancy and childbirth? 13. Using Table 8.1 as a guide, select the three ways that are easiest for you to distinguish a female from a male pelvis.
8.6 Lower Limb (Extremity)
OBJECTIVE
- Identify the bones of the lower limb and their principal markings.
Each lower limb (lower extremity) has 30 bones in four locations— (1) the femur in the thigh; (2) the patella (kneecap); (3) the tibia and fibula in the leg; and (4) the 7 tarsals in the tarsus (ankle), the 5 meta- tarsals in the metatarsus, and the 14 phalanges (bones of the digits) in the foot (see Figures 8.11 and 8.13 ).
Skeleton of the Thigh—Femur and Patella
Femur The femur , or thigh bone, is the longest, heaviest, and strongest bone in the body (Figure 8.11 ). Its proximal end articulates with the acetabulum of the hip bone. Its distal end articulates with
8.6 Lower Limb (Extremity) 249
anterior surface. Just superior to the medial epicondyle is the adduc- tor tubercle, a roughened projection that is a site of attachment for the adductor magnus muscle.
Patella The patella (= little dish), or kneecap, is a small, triangular bone located anterior to the knee joint ( Figure 8.12 ). The broad proximal end of this sesamoid bone, which develops in the tendon of the quadriceps femoris muscle, is called the base; the pointed distal end is referred to as the apex. The posterior surface contains two articular facets, one for the medial condyle of the femur and another for the lateral condyle of the femur. The patellar ligament attaches the patella to the tibial tuberosity. The patellofemoral joint, between the posterior surface of the patella and the patellar surface of the femur, is the intermediate component of the tibiofemoral (knee) joint. The patella increases the leverage of the tendon of the quadriceps femoris muscle, maintains the position of the tendon when the knee is bent (flexed), and protects the knee joint.
POINT OF COMPARISON FEMALE MALE
Pelvic outlet Wider. Narrower. Ischial tuberosity Shorter, farther apart, and more medially projecting.
Longer, closer together, and more laterally projecting.
Right lateral views
Sacrum
Greater sciatic notch
Ilium
Sacrum
Iliac crest
Inferior views
Ischial tuberosity Pelvic outlet Ischial tuberosity Pelvic outlet
Clinical Connection
Patellofemoral Stress Syndrome
Patellofemoral stress syndrome (runner’s knee) is one of the most common problems runners experience. During normal flexion and exten- sion of the knee, the patella tracks (glides) superiorly and inferiorly in the groove between the femoral condyles. In patellofemoral stress syn- drome, normal tracking does not occur; instead, the patella tracks later- ally as well as superiorly and inferiorly, and the increased pressure on the joint causes aching or tenderness around or under the patella. The pain typically occurs after a person has been sitting for a while, especially aft er exercise. It is worsened by squatting or walking down stairs. One cause of runner’s knee is constantly walking, running, or jogging on the same side of the road. Other predisposing factors include running on hills, running long distances, and an anatomical deformity called genu valgum , or knock-knee (see the Medical Terminology section at the end of the chapter).
250 CHAPTER 8 The Skeletal System: The Appendicular Skeleton
form the lateral and medial tibiofemoral (knee) joints. The inferior sur- face of the lateral condyle articulates with the head of the fibula. The slightly concave condyles are separated by an upward projection called the intercondylar eminence ( Figure 8.13b ). The tibial tuberosity on the anterior surface is a point of attachment for the patellar ligament. Infe- rior to and continuous with the tibial tuberosity is a sharp ridge that can be felt below the skin, known as the anterior border (crest) or shin. The medial surface of the distal end of the tibia forms the medial malleolus (mal-LE--ō-lus = hammer). This structure articulates with the talus of the ankle and forms the prominence that can be felt on the medial surface of the ankle. The fibular notch ( Figure 8.13c ) articulates
Skeleton of the Leg—Tibia and Fibula
Tibia The tibia , or shin bone, is the larger, medial, weight-bearing bone of the leg ( Figure 8.13 ). The term tibia means flute, because the tibial bones of birds were used in ancient times to make musical instruments. The tibia articulates at its proximal end with the femur and fibula, and at its distal end with the fibula and the talus bone of the ankle. The tibia and fibula, like the ulna and radius, are connected by an interosseous membrane. The proximal end of the tibia is expanded into a lateral condyle and a medial condyle. These articulate with the condyles of the femur to
FIGURE 8.11 Right femur in relation to the hip bone, patella, tibia, and fibula.
The acetabulum of the hip bone and head of the femur articulate to form the hip joint.
Greater trochanter
Linea aspera
Gluteal tuberosity
Lateral epicondyle
Lateral condyle Fibula
Intercondylar fossa
Hip bone
Neck
Head
Intertrochanteric Line Crest
Body (shaft)
Femur
MEDIAL
Lesser trochanter
Medial epicondyle
Adductor tubercle
Patella
Tibia
Medial condyle
Greater trochanter
Lateral epicondyle Lateral condyle
Fibula
(a) Anterior view (b) Posterior view
Femur
252 CHAPTER 8 The Skeletal System: The Appendicular Skeleton
FIGURE 8.13 Right tibia and fibula in relation to the femur, patella, and talus.
The tibia articulates with the femur and fibula proximally, and with the fibula and talus distally.
Lateral condyle Head
Fibula
Lateral malleolus
Femur
Intercondylar eminence
Medial condyle
Tibial tuberosity
Tibia
Interosseous membrane
Anterior border (crest)
Medial malleolus
MEDIAL
Talus Calcaneus
Patella
Lateral condyle
Fibula
Head
Lateral malleolus
(a) Anterior view (b) Posterior view
Tibia Fibula
MNEMONIC for location of tibia and fibula: The fibu LA is LA teral.
Clinical Connection
Bone Graft ing
Bone grafting generally consists of taking a piece of bone, along with its periosteum and nutrient artery, from one part of the body to replace miss- ing bone in another part of the body. The transplanted bone restores the
blood supply to the transplanted site, and healing occurs as in a fracture. The fibula is a common source of bone for grafting because even after a piece of the fibula has been removed, walking, running, and jumping can be normal. Recall that the tibia is the weight-bearing bone of the leg.
8.6 Lower Limb (Extremity) 253
Tibia (^) Fibular notch
ANTERIOR
Medial malleolus (c) Lateral view of distal end of tibia
View
Q Which leg bone bears the weight of the body?
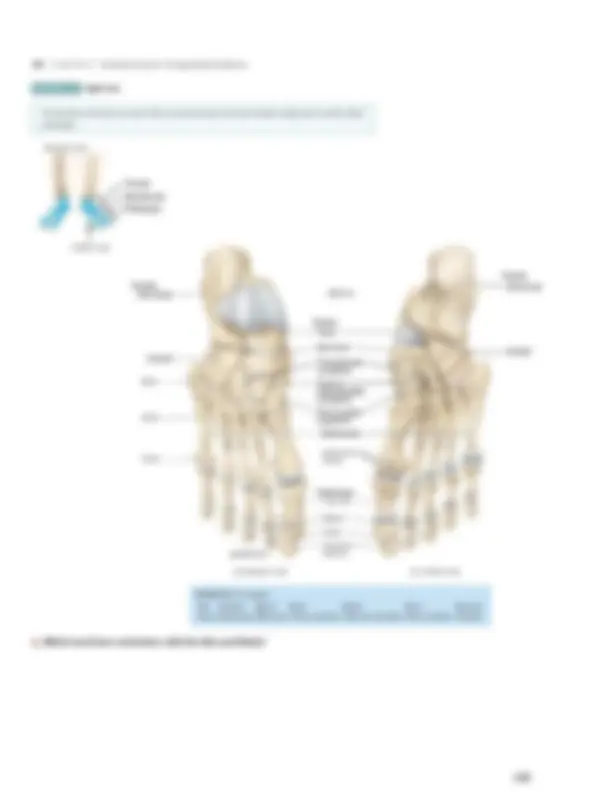
ankle bone) and calcaneus (kal-KA--nē-us = heel), located in the pos- terior part of the foot. The calcaneus is the largest and strongest tarsal bone. The anterior tarsal bones are the navicular (na-VIK-ū-lar = like a little boat), three cuneiform bones (KŪ-nē-i-form = wedge- shaped) called the third (lateral), second (intermediate), and first (medial) cuneiforms , and the cuboid (KŪ-boyd = cube-shaped). (A mnemonic to help you remember the names of the tarsal bones is included in Figure 8.14 .) Joints between tarsal bones are called intertarsal joints. The talus, the most superior tarsal bone, is the only bone of the foot that articulates with the fibula and tibia. It articulates on one side with the medial malleolus of the tibia and on the other side with the lateral malleolus of the fibula. These articulations form the talocrural (ankle) joint. During walking, the talus transmits about half the weight of the body to the calcaneus. The remainder is transmitted to the other tarsal bones. The metatarsus , the intermediate region of the foot, consists of five metatarsal bones numbered I to V (or 1–5) from the medial to lat-eral position ( Figure 8.14 ). Like the metacarpals of the palm of the hand, each metatarsal consists of a proximal base, an intermediate shaft, and a distal head. The metatarsals articulate proximally with the first, second, and third cuneiform bones and with the cuboid to form the tarsometatarsal joints. Distally, they articulate with the proximal row of phalanges to form the metatarsophalangeal joints. The first metatarsal is thicker than the others because it bears more weight.
Clinical Connection
Fractures of the Metatarsals
Fractures of the metatarsals occur when a heavy object falls on the foot or when a heavy object rolls over the foot. Such fractures are also common among dancers, especially ballet dancers. If a ballet dancer is on the tip of her toes and loses her balance, the full body weight is placed on the meta- tarsals, causing one or more of them to fracture.
The phalanges comprise the distal component of the foot and resemble those of the hand both in number and arrangement. The toes are numbered I to V (or 1–5) beginning with the great toe, from medial to lateral. Each phalanx (singular) consists of a proximal base, an intermediate shaft, and a distal head. The great or big toe
(hallux; HAL-eks) has two large, heavy phalanges called proximal and distal phalanges. The other four toes each have three phalanges— proximal, middle, and distal. The proximal phalanges of all toes articulate with the metatarsal bones. The middle phalanges of toes (II–V) articulate with their distal phalanges, while the proximal phalanx of the great toe (I) articulates with its distal phalanx. Joints between phalanges of the foot, like those of the hand, are called interphalangeal joints.
Arches of the Foot
The bones of the foot are arranged in two arches that are held in posi- tion by ligaments and tendons ( Figure 8.15 ). The arches enable the foot to support the weight of the body, provide an ideal distribution of body weight over the soft and hard tissues of the foot, and provide leverage while walking. The arches are not rigid; they yield as weight is applied and spring back when the weight is lifted, thus storing energy for the next step and helping to absorb shocks. Usually, the arches are fully developed by age 12 or 13. The longitudinal arch has two parts, both of which consist of tar- sal and metatarsal bones arranged to form an arch from the anterior to the posterior part of the foot. The medial part of the longitudinal arch, which originates at the calcaneus, rises to the talus and descends through the navicular, the three cuneiforms, and the heads of the three medial metatarsals. The lateral part of the longitudinal arch also be- gins at the calcaneus. It rises at the cuboid and descends to the heads of the two lateral metatarsals. The medial portion of the longitudinal arch is so high that the medial portion of the foot between the ball and heel does not touch the ground when you walk on a hard surface. The transverse arch is found between the medial and lateral aspects of the foot and is formed by the navicular, three cuneiforms, and the bases of the five metatarsals. As noted earlier, one function of the arches is to distribute body weight over the soft and hard tissues of the body. Normally, the ball of the foot carries about 40% of the weight and the heel carries about 60%. The ball of the foot is the padded portion of the sole superficial to the heads of the metatarsals. When a person wears high-heeled shoes, however, the distribution of weight changes so that the ball of the foot may carry up to 80% and the heel 20%. As a result, the fat pads at the ball of the foot are damaged, joint pain develops, and structural changes in bones may occur.