Download COPD ABG gas exchange and more Study notes Medical Genetics in PDF only on Docsity!
Linda Felver
The human body requires precise control of multiple physiologic processes for optimal function. The concentration of hydrogen ions in body fluids influences cellular function, and, thus, organ, system, and whole person function. An abnormal hydrogen ion concentration impairs cellular and organ function and can be fatal. The body maintains the hydrogen ion concentration within the normal range by continuously making adjustments through specific processes. Nurses providing care to acutely and chronically ill patients must understand these processes to optimize their function. This concept presents an analysis of acid–base balance, including the recognition and management of acid–base imbalances when they occur.
DEFINITION
For the purposes of this concept presentation, acid–base balance is defined
as the process of regulating the pH, bicarbonate concentration, and partial
pressure of carbon dioxide of body fluids. The definitions of acid and base
are the foundation for the concept of acid–base balance. An acid is a
substance that releases hydrogen ions (H+), and a base is a substance that
takes up H+. The most important base in the body is bicarbonate (HCO 3 −^ ). The pH of a solution, technically defined later in this concept presentation, is a measure of its degree of acidity. A low pH means the solution is acidic; a high pH means it is basic (alkaline). Acid–base balance is a dynamic interplay between three processes: acid
production or intake, acid buffering, and acid excretion. Acid production is
the generation of acid through cellular metabolism. Our cells continuously generate two kinds of acid during metabolism: carbonic acid (H 2 CO 3 ) and metabolic acids. Although the chemical structures of metabolic acids vary, both normal and abnormal types of cellular metabolism generate metabolic
acids. Occasionally, acid intake occurs, which involves entry into the body of
acids or substances that the body converts to acids (acid precursors). Acid
buffering is a process by which body fluids resist large changes in pH when
acids or bases are added or removed. Body fluids normally have buffers, which are pairs of chemicals that take up H+^ or release it to keep pH in the
normal range. Acid excretion is the removal of acid from the body. These
concepts are described in greater detail later in this concept presentation.
Acid–base balance is described as a dynamic interplay because acid production is occurring constantly, the body fluids constantly have cellular acids added to them that must be buffered to preserve function, and the acid excretion mechanisms must function continuously to keep acids from accumulating in the body. Optimal acid–base balance keeps the pH of the blood and body fluids within the normal physiologic range (7.35 to 7.45 for adults).^1
SCOPE
Considered conceptually, the scope of acid–base balance is on a continuum from acidotic (lower than normal pH) on one end to optimal balance (normal pH and other parameters) in the middle and alkalotic (higher than normal pH) on the other end ( Fig. 7.1 ). These link to three categories associated with this concept: optimal acid–base balance and two types of disrupted acid–base balance—acidosis (too much acid) and alkalosis (too little acid). The term acid–base imbalance often is used to indicate disrupted acid–base balance.
NORMAL PHYSIOLOGICAL PROCESS
The processes whose dynamic interplay is involved in acid–base balance are acid production, acid buffering, and acid excretion. When optimal acid–base balance is occurring, the buffers are not overwhelmed by the amount of acid that is generated and acid excretion keeps pace with acid production. The blood pH and other measures of acid–base status are in the normal range (7.35 to 7.45 for adults; a wider range for infants). This section explains these functions in detail. The process is illustrated in Fig. 7..
Acid Production
Cellular metabolism continuously generates carbonic acid and metabolic acids. Increased cellular metabolism produces more of these acids. FIG. 7.1 Scope of Concept of Acid–base Balance Ranges from Optimal Balance to Acidotic and Alkalotic Imbalances. Carbonic Acid Production Cellular metabolism generates carbonic acid (H 2 CO 3 ) in the form of carbon dioxide (CO 2 ) and water (H 2 O). The enzyme carbonic anhydrase in
This process could decrease the available bicarbonate and increase the concentration of carbonic acid, but normally the 20:1 ratio of bicarbonate to carbonic acid is restored immediately because the lungs excrete the carbonic acid as CO 2 and water. Most of the function of bicarbonate buffers in normal physiology is buffering metabolic acid. Bicarbonate buffers cannot buffer carbonic acid because carbonic acid is part of the buffer. If too much metabolic acid is present, the plasma bicarbonate concentration decreases below its normal range because so much bicarbonate was used in buffering.^3 FIG. 7.2 Acid Production and Excretion. From Potter, P. A., Perry, A. G., Stockert, P., & Hall, A. [2013]. Fundamentals of nursing. [8th ed.]. St Louis: Mosby. In abnormal circumstances in which too little metabolic acid is present, the carbonic acid portion of the bicarbonate buffer system will release H+. This process simultaneously raises the bicarbonate concentration and may restore the pH. However, if entirely too little metabolic acid is present, the plasma bicarbonate concentration increases above its normal range. Thus, the plasma bicarbonate concentration is an indicator of the metabolic acid status in the blood.
Acid Excretion
The two types of acid produced by cellular metabolism differ in that carbonic acid is converted to gases and metabolic acid is not. The lungs excrete the gaseous form of carbonic acid, and the kidneys excrete metabolic acid. Carbonic Acid Excretion The lungs serve as the excretory organ for carbonic acid. The lungs are not able to excrete metabolic acid because it cannot be converted into a gaseous form. Changes in respiratory rate and depth alter the amount of carbonic acid that is excreted. Hyperventilation (increased rate and depth of respiration) excretes more carbonic acid; hypoventilation (decreased rate and depth of respiration) excretes less carbonic acid. The chemoreceptors influence respiratory rate and depth in response to blood levels of CO 2 and H+^ and, in some situations, oxygen. When the amount of CO 2 increases in
the blood, the chemoreceptors increase the respiratory rate and depth,^1 which excretes more CO 2 and H 2 O (carbonic acid) and helps restore the CO 2 level to its normal range. If the blood has too little CO 2 , the chemoreceptors decrease the respiratory rate and depth, which enables the CO 2 level to rise to its normal range because the cells constantly are
producing it. These are examples of correction: fixing the problem and
returning the blood values to their normal range. Because chemoreceptors respond to H+^ concentration as well as to blood levels of CO 2 , they modify respiratory rate and depth in response to the level of metabolic acid as well as carbonic acid. If too much metabolic acid accumulates, the chemoreceptors trigger hyperventilation (increased respiratory rate and depth).^1 ,^3 This does not correct the problem because the lungs cannot excrete metabolic acid, but hyperventilation removes more carbonic acid from the body, thus making the blood less acidic. The result is too little carbonic acid, which helps balance the excess metabolic acid. The
technical term for this process is compensation: moving the pH toward its
normal range while making other blood values abnormal. If too little metabolic acid is present, the chemoreceptors cause hypoventilation.^4 This compensatory process moves the pH down toward its normal range by allowing too much carbonic acid to help balance the too little metabolic acid. Metabolic Acid Excretion The kidneys excrete metabolic acid but are unable to excrete carbonic acid. They have several mechanisms for excreting metabolic acid. Glomerular filtrate that enters the renal tubules contains HCO 3 −^ from blood. Cells that line the renal proximal tubules perform chemical processes that essentially take H+^ from the blood and secrete it into renal tubular fluid while moving HCO 3 −^ in the opposite direction, from the renal tubules into blood. The A−^ portion of metabolic acids enters renal tubular fluid in the proximal tubules as well. Infants and older adults have reduced ability to excrete large amounts of metabolic acids.^5 ,^6 The secretion of metabolic acid into the renal tubules adds free H+^ to the fluid, which potentially could damage renal cells. However, many of these H+^ combine with other molecules in the renal tubular fluid, and they no longer influence the pH. For example, renal tubular fluid contains buffers,
and an immature renal system that is inefficient in excreting a sudden acid load.^5 In addition, an infant’s metabolic rate is higher than that of an adult. These differences place infants at higher risk for metabolic acidosis, as well as fluid and electrolyte imbalances, compared with older children and adults. Older Adults A normal physiologic change associated with aging is reduced size and function of the kidneys, which play a critical role in maintaining acid–base balance.^6 Despite this age-related gradual loss of nephrons, the kidneys of the older adult typically are able to manage their role in fluid, electrolyte, and acid–base balance under normal circumstances. However, older adults have reduced renal reserve. They are less able to excrete a large acid load renally, and their ability to compensate may be less effective. This makes older adults more susceptible to acid–base disturbances, as well as to fluid and electrolyte imbalances.
VARIATIONS AND CONTEXT
Conceptually, variations in acid–base balance are referred to as acid–base imbalance, of which there are two major categories: acidosis and alkalosis. Each of these categories has two underlying subtypes: respiratory and metabolic ( Fig. 7.3 ). When these conditions are developing, the body attempts to manage the changing acid–base balance through the corrective and compensatory responses described previously. Table 7.1 summarizes the corrective and compensatory responses to disrupted acid–base balance.
Acidosis (Too Much Acid)
In a situation of too much acid, the buffers have been overwhelmed and body fluids have too much acid. Acid excretion is not able to keep up with acid production or intake. Conditions of too much acid are
called acidosis and are given an additional descriptor that explains whether
there is too much carbonic acid or too much metabolic acid. Because the lungs excrete carbonic acid, the condition of too much carbonic acid is
called respiratory acidosis.^1 ,^7 Similarly, because the kidneys excrete
metabolic acid, the condition of too much metabolic acid is called metabolic
acidosis. In some cases of metabolic acidosis, the base bicarbonate has been
lost from the body, which causes relatively too much metabolic acid. In situations of too much acid, the pH is below the normal range (or in the low part of the normal range), and some other measures of acid–base status are abnormal. These laboratory values are explained in the Assessment section. FIG. 7.3 Categories of Acid–Base Imbalances.
Alkalosis (Too Little Acid)
In situations of too little acid, the buffers also are not able to keep the pH in the normal range and body fluids do not have enough acid. Too much of the base HCO 3 −^ has been added to the buffer system or acid excretion is greater
than acid production. Conditions of too little acid are called alkalosis—
either respiratory alkalosis when there is too little carbonic acid
or metabolic alkalosis when there is too little metabolic acid.^1 ,^7 In these
situations of too little acid, the pH is above the normal range (or in the high part of the normal range) and some other measures of acid–base status are abnormal. The Assessment section explains these measures.
CONSEQUENCES
A firm grasp of the physiologic processes that comprise acid–base balance makes it possible to understand the consequences when these processes are disrupted. Acid–base imbalances trigger compensatory mechanisms, as described previously. The time course of those mechanisms has important clinical implications. In addition to triggering compensatory mechanisms, pH changes impair cellular and organ function.
Time Course of Compensatory Mechanisms
Disruptions of acid–base balance cause the blood pH to move outside its normal range. In these situations, the buffers have been overwhelmed and the acid excretion mechanisms must work to keep the pH from reaching the fatal limits. If the pH falls abnormally low from too much acid, both the lungs and the kidneys will excrete more acid, even though only one of these organs will be excreting the type of acid that is excessive. The other organ is compensating. Depending on the time course and the severity of the problem, the disruption may be uncompensated, partially compensated, or fully compensated.^1
Respiratory and Renal Responses to Disrupted Acid–Base Balance Stimulus Respiratory Response Renal Response Too little metabolic acid (metabolic alkalosis) Compensation: Hypoventilation Cause of Problem: More bicarbonate than kidneys can excrete (too little metabolic acid) Correction: Decreased secretion of H+ Less NH^3 production As explained in the previous section, if a problem with the respiratory system disrupts acid–base balance and the lungs are unable to correct it, renal compensatory mechanisms adjust the pH toward normal. It takes several days for renal compensatory mechanisms to become clinically significant^1 ,^7 ; therefore, a short-lived respiratory acidosis or alkalosis will not become compensated. Rapid treatment of an acute respiratory acidosis will correct the problem before renal compensation can occur. On the other hand, people who have chronic respiratory acidosis or an acute episode that lasts several days do develop some degree of renal compensation, either partial or full. Episodes of respiratory alkalosis occur from hyperventilation and it is uncommon, but possible, for them to last long enough for renal compensation to occur. Analogously, if a problem with the kidneys disrupts acid–base balance and the kidneys are unable to correct it, respiratory compensatory mechanisms adjust the pH toward normal.^7 Respiratory compensation begins within a few minutes after the pH becomes abnormal, so it is common to have some degree of compensation for a disruption of acid–base balance that involves too much or too little metabolic acid. When the disruption is severe, it will be only partially compensated.^1 ,^7 In cases of metabolic alkalosis (too little
metabolic acid), compensatory hypoventilation is limited by the respiratory drive for oxygen, so that full compensation usually does not occur.^8 It is important to realize that even if compensatory mechanisms do not return the pH to the normal range, they do prevent pH from becoming more abnormal.
Impaired Cellular and Organ Function
Disruptions of acid–base balance alter cell function, especially in the brain. The disorders involving carbonic acid (respiratory acidosis and alkalosis) generally cause more neurologic signs and symptoms than those involving metabolic acid (metabolic acidosis and alkalosis).^1 ,^9 This difference occurs because CO 2 from carbonic acid crosses the blood-brain barrier easily and changes the pH of cerebrospinal fluid rapidly. Metabolic acid and HCO 3 −^ cross the blood-brain barrier with difficulty and produce fewer neurologic manifestations or cause them more slowly. The enzymes inside cells work most effectively when pH is in the normal range. Abnormal extracellular pH can cause intracellular pH to change, especially with respiratory acidosis and alkalosis. The resulting change in enzyme activity contributes to cell dysfunction. Acidosis decreases the level of consciousness (LOC). With alkalosis, initial excitation may occur, followed by decreased LOC if the pH increase becomes more severe.^1 In addition to brain cell dysfunction that causes altered LOC and other neurologic manifestations, cardiac cell dysfunction from acid–base imbalances can cause dysrhythmias.^1 Concurrent potassium imbalances caused by acid– base imbalances also cause cardiac dysrhythmias.
RISK FACTORS
Populations at Risk
All individuals, regardless of genetics, culture, age, or socioeconomic status, need optimal acid–base balance for physiologic function. From a population perspective, those at greatest risk for acid–base disturbances are the very young and the very old. Preterm infants are at great risk for acid–base disturbances due to immature lungs, kidneys, thermoregulation, and metabolic processes; the degree of risk is largely related to the weight and gestational age at the time of birth. Term infants also have greater risk than adults due to immature kidneys and elevated metabolic rate.^5
populations for ketoacidosis are people who do not have enough carbohydrate intake and people with alcohol use disorder.^13 ,^14 In addition to the production of excessive metabolic acid within the body, excessive intake of acid or acid precursors also causes metabolic acidosis. Although metabolic acidosis from intake of acid or acid precursors is less common, it is significant clinically in people who accidentally ingest boric acid (intended for ant poisoning) or who drink methanol, hand sanitizer (contains isopropanol and also may be contaminated with methanol), or antifreeze (an acid precursor).^15 -^17 B O X 7. 1 C o m m o n U n d e r l y i n g C o n d i t i o n s L e a d i n g T o A c i d – B a s e I m b a l a n c e COPD, Chronic obstructive pulmonary disease. Respiratory Acidosis (Too Much Carbonic Acid) Alveolar Hypoventilation 1.• Type B COPD (chronic bronchitis) 2.• End-stage type A COPD (emphysema) 3.• Severe asthma episode 4.• Bacterial pneumonia 5.• Pulmonary edema Ineffective Respiratory Pump 1.• Guillain–Barré syndrome Central Suppression of Respiration 1.• Opioid overdose Metabolic Acidosis (Too Much Metabolic Acid) Excessive Production or Intake of Metabolic Acid 1.• Diabetic ketoacidosis 2.• Starvation ketoacidosis 3.• Alcohol-related ketoacidosis 4.• Lactic acidosis (from tissue anoxia) 5.• Thyroid storm Decreased Excretion of Metabolic Acid 1.• Oliguria from any cause Loss of Bicarbonate 1.• Prolonged diarrhea 2.• Draining intestinal or pancreatic fistula Respiratory Alkalosis (Too Little Carbonic Acid) Hyperventilation 1.• Acute hypoxia 2.• Acute pain
3.• Acute anxiety or emotional distress 4.• Central stimulation of respiration by inflammation from head injury or meningitis Metabolic Alkalosis (Too Little Metabolic Acid) Gain of Base (Bicarbonate) 1.• Excessive ingestion or infusion of NaHCO 3 2.• Massive blood transfusion (citrate metabolized to ) 3.• Diuretic therapy (contraction alkalosis) Excessive Excretion of Metabolic Acid 1.• Repeated vomiting 2.• Mineralocorticoid excess In summary, risk factors for excessive production or intake of metabolic acid include the risk factors for ketoacidosis or poisoning with acids or substances the body converts to acid. All of these situations place people at risk for metabolic acidosis. The cells cannot stop producing metabolic acid, so decreased acid production is not a risk factor for acid–base imbalance. Altered Acid Buffering Due to Loss or Gain of Bicarbonate The base bicarbonate is a component of the major buffer system that buffers metabolic acids. It is possible to lose or gain bicarbonate and, thus, alter the buffering capacity. People who lose a significant amount of bicarbonate, such as through prolonged diarrhea, lose buffering capacity and have
relatively too much metabolic acid. Thus, bicarbonate loss causes metabolic
acidosis.^1 ,^7 Conversely, gaining a significant amount of bicarbonate, such as by ingesting baking soda (sodium bicarbonate) as an antacid or by receiving excessive intravenous (IV) sodium bicarbonate, makes too much bicarbonate buffer available, creating too little metabolic acid. Thus,
bicarbonate gain causes metabolic alkalosis.^1 ,^8 In summary, risk factors for
altered acid buffering include prolonged diarrhea and excessive sodium bicarbonate intake in people of any age.^10 These conditions place them at risk for metabolic acidosis or metabolic alkalosis. Altered Acid Excretion Cellular metabolism generates two types of acid that are excreted by two different organ systems. For this reason, altered acid excretion occurs in many disease processes that affect lung and kidney function. Carbonic acid excretion occurs by gas exchange in the lung alveoli followed by exhalation;
vomiting,^25 which removes hydrochloric acid. Vomiting also triggers bicarbonate retention by the kidneys, which alters the buffering capacity and contributes to the resulting metabolic alkalosis. In summary, risk factors for altered acid excretion include respiratory or other conditions that interfere with the ability to excrete enough carbonic acid, conditions causing hyperventilation that excretes too much carbonic acid, kidneys that are unable to excrete enough metabolic acid, and situations in which the kidneys or repeated episodes of vomiting remove too much metabolic acid from the body.^8 Abnormal Shift of H+^ into Cells Factors that shift substantial numbers of H+^ into cells can cause too little acid to be in the blood. The most common example in this category of risk factors is hypokalemia (abnormally low plasma potassium concentration).^8 When hypokalemia is present, some potassium ions (K+) leave cells and H+^ enter cells to maintain a balance of electrical charge. The result is too little metabolic acid in the blood, known as metabolic alkalosis. The primary risk factor for abnormal shift of H+^ into cells is hypokalemia. Risk factors for hypokalemia are discussed in Concept 6, Fluid and Electrolytes.
ASSESSMENT
Disruptions of acid–base balance almost always result from other conditions. For this reason, assessments of acid–base status usually are performed in the context of other conditions.
History
Clinical manifestations associated with disrupted acid–base balance often are caused by an underlying condition and associated fluid and electrolyte imbalances. Acid–base imbalances cause nonspecific signs such as decreased LOC that have many possible causes. It is critical that nurses consider presenting symptoms in the context of other current health conditions. The history focuses on the respiratory, renal, or other conditions that could cause the acid–base problem. The standard questions for any history apply and are not repeated here. Other areas to explore in the history include the following: a recent history of vomiting or diarrhea
(repeated vomiting causes metabolic alkalosis; prolonged diarrhea causes metabolic acidosis); use of heartburn or indigestion medications (a few days of baking soda/sodium bicarbonate ingestion can cause metabolic alkalosis); food insecurity; recent attempts to lose weight and methods employed (high-fat, low-carbohydrate diet or fasting predispose to starvation ketoacidosis); and use of medications, dietary supplements, recreational drugs, and alcohol.^26 -^29
Examination Findings
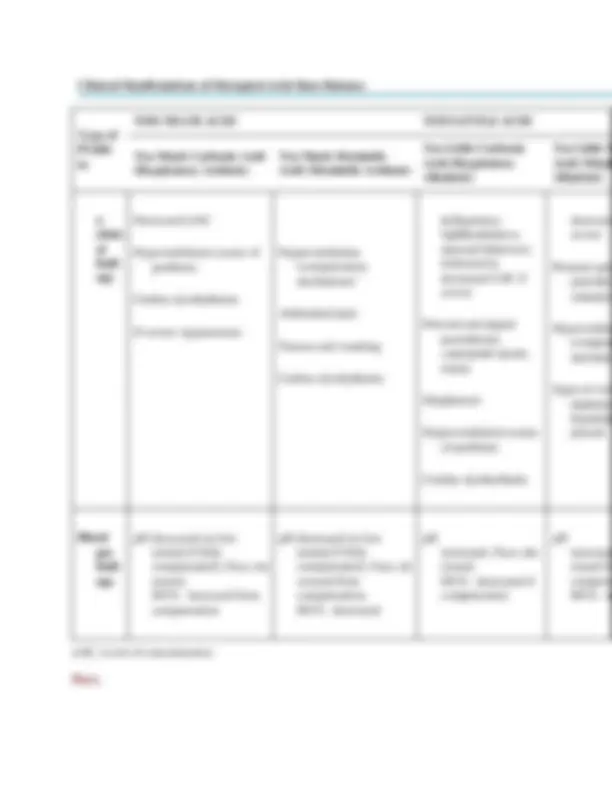
Unless the acid–base imbalance is severe, specific signs and symptoms of disrupted acid–base balance often are overshadowed by the clinical manifestations of the underlying cause. For example, in a person who has type B COPD (chronic bronchitis), the dyspnea and excessive mucus production usually are more obvious than the mild drowsiness from partially compensated respiratory acidosis. With severe acute asthma, the chest tightness, coughing, wheezing, use of accessory respiratory muscles, and poor oxygenation typically overshadow the manifestations of acute respiratory acidosis.^1 People who have end-stage kidney disease experience many clinical manifestations from this chronic oliguric condition that predominate over lethargy from the metabolic acidosis that may occur between dialysis sessions, unless it becomes severe.^1 With substantial rapid changes of pH, such as with ketoacidosis, dramatic changes in LOC can overshadow the signs and symptoms of the underlying condition. For example, a person who develops DKA typically will have been experiencing the polyuria, polydipsia, polyphagia, and weight loss of hyperglycemia before the onset of ketoacidosis. These manifestations often are realized only in retrospect, after abdominal pain and decreased LOC from the ketoacidosis have become the focus of attention and the metabolic acidosis is resolved. Table 7.2 presents signs and symptoms of the various disruptions of acid–base balance. These manifestations arise from the impaired cellular and organ function described previously in this concept analysis. Decreased LOC occurs on a continuum from decreased attention span and drowsiness on one end to stupor and coma on the other. Interpretation of assessment findings may be complicated by the presence of fluid and electrolyte imbalances (see Concept 6, Fluid and Electrolytes).
Clinical Manifestations of Disrupted Acid–Base Balance Type of Proble m
TOO MUCH ACID TOO LITTLE ACID
Too Much Carbonic Acid (Respiratory Acidosis) Too Much Metabolic Acid (Metabolic Acidosis) Too Little Carbonic Acid (Respiratory Alkalosis) Too Little M Acid (Metab Alkalosis) n clinic al findi ngs Decreased LOC Hypoventilation (cause of problem) Cardiac dysrhythmias If severe: hypotension Hyperventilation (compensatory mechanism) Abdominal pain Nausea and vomiting Cardiac dysrhythmias belligerence, lightheadedness, unusual behaviors; followed by decreased LOC if severe Perioral and digital paresthesias, carpopedal spasm, tetany Diaphoresis Hyperventilation (cause of problem) Cardiac dysrhythmias decrease severe Perioral and paresthes carpoped Hypoventila (compen mechanis Signs of volu depletion hypokale present Blood gas findi ngs pH decreased (or low normal if fully compensated); P aco 2 inc reased; HCO 3 −^ increased from compensation pH decreased (or low normal if fully compensated); P aco 2 de creased from compensation; HCO 3 −^ decreased pH increased; P aco 2 dec reased; HCO 3 −^ decreased if compensation pH increased reased fr compens HCO 3 −^ in LOC, Level of consciousness. Paco 2
Paco 2 is the partial pressure of CO 2 in the arterial blood. It indicates how
well the lungs are excreting carbonic acid (CO 2 and H 2 O).^10 The normal
range of Paco 2 is 35 to 45 mm Hg (4.7 to 6.0 kilopascals [kPa]) for adults
(lower in infants). Increased Paco 2 level indicates CO 2 accumulation in the
blood (too much carbonic acid) caused by primary or compensatory
hypoventilation; decreased Paco 2 level indicates excessive CO 2 excretion
(too little carbonic acid) caused by primary or compensatory hyperventilation. HCO 3 −^ Concentration The serum HCO 3 −^ concentration indicates how well the kidneys are excreting metabolic acid.^10 The normal adult range is 22 to 26 mEq/L (22 to 26 mmol/L); the range is lower in infants. Increased HCO 3 −^ concentration indicates that the blood has too little metabolic acid; decreased HCO 3 −^ concentration indicates that the blood has too much metabolic acid. Base Excess Base excess, which normally ranges from −2 to +2 mmol/L, is an indicator of how well the buffers are managing metabolic acid.^1 Values less than − mmol/L (negative base excess) indicate too much metabolic acid; values greater than +2 mmol/L indicate too little metabolic acid. When people develop metabolic acidosis, clinicians may calculate other values, such as the anion gap and the osmolal gap, to assist in diagnosing the specific cause.^3 ,^17 ,^32 C O R E C O M P E T E N C I E S Acid–Base Balance 1.• Demonstrate clinical judgment founded on broad knowledge of acid–base balance. 2.• Using a person-centered approach, teach individuals and families regarding prevention and management of acid–base imbalances. 3.• Select, interpret, and act upon assessments related to acid–base balance. 4.• Using a person-centered approach, implement interventions and evaluate the plan of care to address individual patient and family needs related to acid–base balance. 5.• Collaborate with the interprofessional team to provide patient safety and optimal management of acid–base imbalances.
CLINICAL MANAGEMENT