Download CPJE PEDIATRICS sample questions and more Cheat Sheet Pharmacy in PDF only on Docsity!
Pediatrics
Alyssa Wu, Pharm.D., BCPPS, AE-C
Immersive Board Review
Learning Objectives
2024 Rx4Success
• Explain after birth neonatal treatments and ongoing
supplementation
• Describe over the counter treatments for pediatric patients
• Analyze empiric treatment for common pediatric conditions
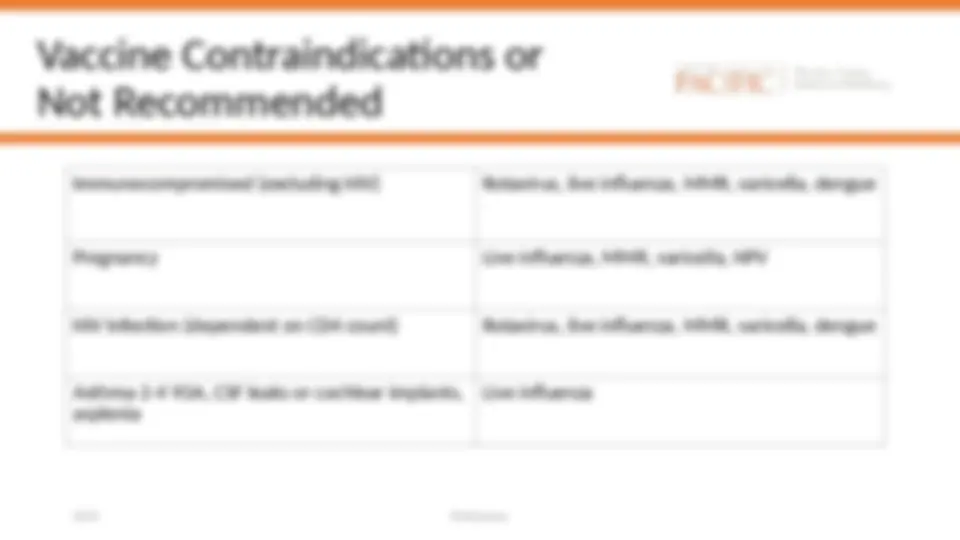
• Evaluate drugs not recommended for use in the pediatric
population
• Recall drugs with different indications in pediatrics than adults
• Summarize the CDC vaccine schedule
• Discuss oral medications that require refrigeration
• List intravenous medications that do not require refrigeration
Eyes and Thighs
2024 Rx4Success
• You are processing orders as an inpatient pharmacist in a neonatal
intensive care unit. Vitamin K is ordered intramuscularly and
erythromycin ointment to be applied topically to the eyes.
• Why are these two medications ordered for every neonate?
Eyes and Thighs
2024 Rx4Success
Brand Generic Dosing DDIs Indication ADRs Storage Preparation Clinical
Caveats
Phytonadione Vitamin K 0.5-1 mg IM
once at birth
None Prevention of
vitamin K
deficiency
bleeding
Injection site
pain
Protect
from light
IM undiluted
Erythromycin
ophthalmic
ointment
Topical to
both eyelids
once
None Prevention of
eye
infections
Eye irritation Do not flush eye
following
instillation
Supplementation After Birth
2024 Rx4Success
American Academy of Pediatrics Recommendations:
● Vitamin D: 400 units for all solely breastfed babies
● Babies taking less than 27 oz of standard formula may also
need supplementation
○ Goal level: >
● Iron: 1-3 mg elemental iron/kg/day for all solely breastfed
babies at 4 months of age
Supplementation After Birth
Brand Generic Dosing DDIs Indication ADRs Storage Counseling
Points
Cholecalciferol Vitamin D Prevention: 400
units daily oral
beginning in the
first few days of
life
None Vitamin D
deficiency
prevention and
treatment
None Do not freeze,
protect from
light
Administer with
accurate
measuring
device, do not
use a teaspoon
Ferrous sulfate Iron Prevention: 1-
mg elemental
iron/kg/day oral
Antacids may
decrease
absorption; iron
may decrease
levothyroxine,
cefdinir and
phosphate
supplements
Iron deficiency
prevention and
treatment
Dark stools,
abdominal pain,
nausea,
constipation
Store out of
children’s
reach and in
child resistant
containers
(leading cause
of fatal
poisoning)
Do not
administer with
milk or milk
products
Can administer
with food to
decrease ADRs
Do not crush EC
or film-coated
tablets
OTC and Commonly Used Products
2024 Rx4Success
Mild Pain and Fever
• Acetaminophen (Tylenol): 10-15 mg/kg/dose (max: 500-650mg per dose), NTE 75
mg/kg/day or 4 grams/day (whichever is less)
• Ibuprofen (Advil, Motrin): 5-10 mg/kg/dose (max: 600-800mg per dose), avoid in
patients <6 months of age due to risk of nephrotoxicity
• Aspirin: not recommended in patients <16 YOA due to risk of Reye’s syndrome
Intestinal Gas
• Simethicone: 20 mg, 1-4 times a day prn
Nasal Dryness/Congestion:
• Intranasal saline solution: 2-6 drops per nostril prn
• The FDA does not recommend use of OTC cough and cold medications in patients <
YOA
OTC and Commonly Used Products
2024 Rx4Success
Constipation
● Polyethylene glycol (Miralax): 0.2-0.8 g/kg/day (max dose: 17 g or 1 capful)
● Docusate (Dulcolax): 5 mg/kg/day (max dose: 150mg)
● Sennoside (Senna): 2.2mg-16.6mg based on age
Diarrhea
● Bismuth subsalicylate should not be used due to the risk of Reye’s syndrome
● Loperamide should not be used in patients <2 YOA due to the risk of respiratory
depression and serious cardiac adverse reactions; 1-4mg based on age
Nausea
● Ondansetron: 0.15 mg/kg (max dose: 4 mg), ODT tab available (not OTC but
commonly used)
Common Conditions -
Bacterial Meningitis
2024 Rx4Success
What is the most likely treatment for bacterial meningitis in a patient
less than 1 month old?
A. Ampicillin + cefotaxime
B. Vancomycin + 3rd generation cephalosporin
C. Ampicillin + gentamicin
D. A and C
E. All of the above
Common Conditions -
Bacterial Meningitis
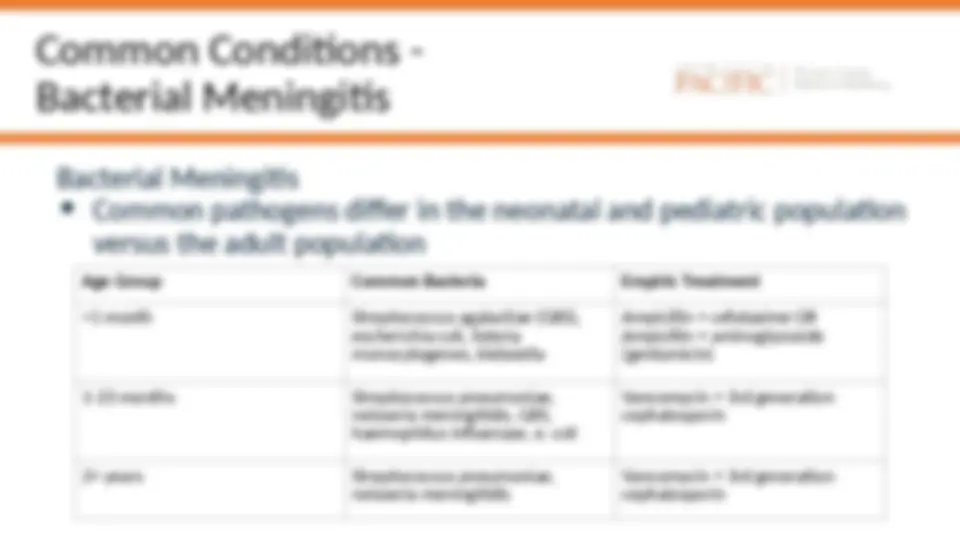
Bacterial Meningitis
• Common pathogens differ in the neonatal and pediatric population
versus the adult population
Age Group Common Bacteria Empiric Treatment <1 month Streptococcus agalactiae (GBS), escherichia coli, listeria monocytogenes, klebsiella Ampicillin + cefotaxime OR Ampicillin + aminoglycoside (gentamicin) 1-23 months Streptococcus pneumoniae, neisseria meningitidis, GBS, haemophilus influenzae, e. coli Vancomycin + 3rd generation cephalosporin 2+ years Streptococcus pneumoniae, neisseria meningitidis Vancomycin + 3rd generation cephalosporin
Common Conditions - RSV
2024 Rx4Success
Which of the following patients should receive palivizumab or
nirsevimab during the RSV season?
A. Premature infant <30 weeks gestation
B. Premature infant born <32 weeks gestation with chronic lung
disease who is <1 year of age
C. Infants <2 years of age with certain heart conditions
D. All patients under the age of 18
Common Conditions - RSV
2024 Rx4Success
Respiratory Syncytial Virus (RSV)
● Very common virus that infects almost all children by the age of 2
● Can cause severe complications in premature babies, neonates and
immunocompromised children
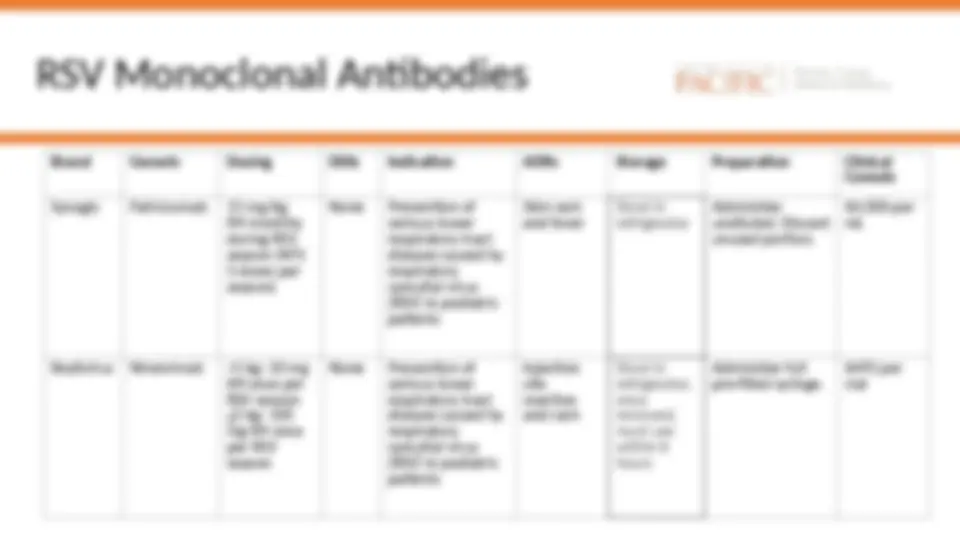
RSV Monoclonal Antibodies
Brand Generic Dosing DDIs Indication ADRs Storage Preparation Clinical Caveats Synagis Palivizumab 15 mg/kg IM monthly during RSV season (NTE 5 doses per season) None Prevention of serious lower respiratory tract disease caused by respiratory syncytial virus (RSV) in pediatric patients Skin rash and fever Store in refrigerator Administer undiluted. Discard unused portion. $4,000 per mL Beyfortus Nirsevimab <5 kg: 50 mg IM once per RSV season
5 kg: 100 mg IM once per RSV season None Prevention of serious lower respiratory tract disease caused by respiratory syncytial virus (RSV) in pediatric patients Injection site reaction and rash Store in refrigerator, once removed, must use within 8 hours Administer full pre-filled syringe. $495 per vial
Common Conditions - Influenza
A. Oseltamavir B. Zanamavir^ C. Peramavir D. Oral treatment of influenza is not recommended
Which of the following is the oral treatment of choice for influenza in
pediatric patients?