Download Critically Ill Midterm Study Guide and more Study Guides, Projects, Research Nursing in PDF only on Docsity!
Critically Ill Midterm Study Guide
Normal Values
*CVP/RAP: 2-8 mmHg
● 10 = fluid overload
● 0 = dehydrated
*CO: 4-8 L/min
*Cl: 2.2-4.
● Cl in cardiogenic shock: 1.5-2.
● Cl irreversible:
<1.5 PAS: 15-30 mmHg
PAD: 4-12 mmHg
*PCWP/LAP: 6-
● 12-18 when the PA cath is in place
○ This allows for compensation (i.e.
ARDS) PAP: 25/10 mmHg
MPAP: 15 mmHg
SVO2: 60-80%
● Low SVO2 = decreased O2 supply or increased O2 demand
● High SVO2 = increased O2 supply or decreased O2 demand
*SVR: 800-1,200 dynes-s/cm
*PVR: <250 dynes-s/cm5 or 160-
SV (contractility): 60-180 cc
ETT cuff pressure: <30 mmHg
Hemodynamic monitoring (15) ● Hemodynamic Monitoring Modalities ○ Invasive and noninvasive hemodynamic monitoring is a major part of a comprehensive assessment of the critically ill patient. The goal in evaluating hemodynamic data is to determine if oxygen supply is meeting oxygen demands. The hemodynamic assessment aids in surveillance and early detection of oxygen imbalance, quantifying the severity of
disease, and as a guide for assessing and adjusting therapies. Traditional hemodynamic monitoring uses specific end points to guide therapies (e.g., mean arterial pressure [MAP], CO, central venous pressure [CVP], pulmonary artery occlusion pressure [PAOP], urine output, pH, and lactate). Newer modalities, such as bedside echocardiography, mixed venous oxygen saturation (SvO 2 ) monitoring, and changes in the arterial pressure waveform, evaluate dynamic indices. Normal hemodynamic values are described in Table 8-1; however, these values only provide a guideline to assist interpretation of assessment findings. The primary goal of hemodynamic monitoring is to assess and trend adequacy of tissue oxygenation and perfusion, rather than to compare a patient’s values to so-called normal parameters. ■ Noninvasive Monitoring - Some critically ill patients can be adequately assessed and managed with noninvasive hemodynamic monitoring. Noninvasive technologies include noninvasive blood pressure (NIBP) measurement, assessment of jugular venous pressure, and frequent assessments of laboratory tests, such as lactate. ● Jugular Venous Pressure - Assessment of the jugular veins provides an estimate of intravascular volume, and it is an indirect measure of CVP. Because the internal jugular vein directly communicates with the right atrium, it can serve as a manometer to provide an estimate of the CVP. Jugular venous distension occurs when the CVP is elevated, which can occur with fluid overload, right ventricular dysfunction, superior vena cava obstruction, and right heart failure ● Lactate - Anything that deprives the tissues of oxygen disrupts the Krebs cycle, resulting in anaerobic metabolism and increased production of lactic acid. Normal arterial lactate levels range from 0.5 to 1.6 mEq/L.^8 In lactic acidosis the lactate level is elevated, commonly 10 to 30 mEq/L. Lactate levels may be measured to determine tissue hypoperfusion in shock, to establish adequacy of resuscitation, and to assist in diagnosis of patients who have metabolic acidosis of unknown cause. The use of lactate levels to guide therapy with a goal to reduce levels 20% every 2 hours can be used in conjunction with other parameters such as MAP, heart rate, urine output, hemoglobin levels, arterial oxygen saturation (SaO 2 ), and central venous oxygen saturation (ScvO 2 ) to manage patients and reduce intensive care unit (ICU) length of stay and ICU and hospital mortality. ○ Indications for Invasive Hemodynamic Monitoring - Invasive methods of hemodynamic monitoring are used to obtain more detailed physiologic information. Common indications for invasive monitoring are outlined in Box 8-1. A comprehensive hemodynamic assessment is used to guide interventions in patients with the following diagnoses: shock, cardiac tamponade, ruptured ventricular septum, heart failure, and right ventricular infarction. In addition, hemodynamic monitoring is used with complex surgical patients to guide therapy and detect complications early. ■ The first step in a hemodynamic assessment is to determine the adequacy of tissue perfusion and whether the patient is in a state of shock that requires fluid
catheter is approximately 35 to 40 cm. Focusing the probe entails rotating, advancing, or withdrawing the probe until the loudest sound is heard from the monitor. ■ Indications ● States of hypoperfusion (hypovolemia, hemorrhagic shock, septic shock) ● Hemodynamic monitoring and evaluation of major end- organ dysfunction ● Differential diagnosis of hypotensive states ● As an adjunct for diagnosis and management of heart failure, cardiogenic shock, valvular dysfunction, ventricular septal rupture, cardiac rupture with tamponade ● Preoperative, intraoperative, and postoperative management of high- risk cardiac patients undergoing surgical procedures ■ Contraindication ● Local disease ○ Esophageal stent ○ Carcinoma of the esophagus or pharynx ○ Previous esophageal surgery ○ Esophageal stricture ○ Esophageal varices ○ Pharyngeal pouc ● Aortic abnormalities ○ Intraaortic balloon pump ○ Coarctation of the aorta ● Systemic ○ Severe coagulopathy ● CO/Cardiac Index (3) ○ Cardiac output = Cardiac Index ■ Heart rate x stroke volume (amount of blood ejected by the heart with each beat) ● SV is affected by preload, afterload, and contractility ○ Preload is the degree of ventricular stretch before the next contraction. The degree of stretch is directly affected by the amount of blood volume present in the ventricles at end- diastole ■ Another way of explaining the mechanism is that within physiologic limits, the heart pumps all of the blood that
is returned by the venous system. Too much end- diastolic volume in the right ventricle can result in congestion of the systemic vasculature, and too much end-diastolic volume in the left ventricle can cause fluid to back up into the pulmonary vasculature. Too little blood at end-diastolic volume results in a reduction in CO. Optimizing preload or ventricular filling is the goal of many therapeutic interventions in critical care. ○ Afterload is the amount of resistance the ventricles must overcome to deliver the SV into the receiving vasculature ■ The left ventricle during systole must create the force necessary to open the aortic valve and overcome the resistance in the systemic circulation. The right ventricle must create enough force to open the pulmonic valve and overcome the 134resistance in the pulmonary circulation ○ Contractility is the strength of myocardial muscle fiber shortening during the systolic phase of the cardiac cycle. It is the force with which the heart propels the SV forward into the vasculature. ■ The preload influences contractility because optimizing the preload ensures maximal stretch of the myocardial fibers according to the Frank-Starling law. Contractility is not directly measured; however, it can be expressed by the calculated values of right or left ventricular stroke work index. ○ The autonomic nervous system has two branches that control the cardiovascular system: the sympathetic and the parasympathetic. Sympathetic nervous system activity enhances myocardial performance by shortening the conduction time through the AV node, enhancing rhythmicity of the AV pacemaker cells and increased myocardial contractility. Parasympathetic nervous system activity via the vagus nerves results in blocking of cardiac action potentials initiated by the sinus node in the atria, thus decreasing heart rate. ○ The cardiovascular system is also regulated by hormonal influences to maintain adequate oxygen delivery to meet the demands of the tissues. Norepinephrine increases the heart rate and myocardial contractility and causes vasoconstriction. Epinephrine produces its effects by stimulating the alpha- adrenergic receptors located in the walls of the arteriole. Additionally, epinephrine is a beta-adrenergic stimulator and may cause vasodilation of arterioles in skeletal muscle. ○ The right atrium secretes atrial natriuretic peptides (ANPs), and the ventricular myocardium secretes brain natriuretic peptides (BNPs) in response to stretch from the heart chambers. ANPs and BNPs cause vasodilation and diuresis and inhibit the sympathetic response and the renin-angiotensin- aldosterone system (RAAS) in an attempt to decrease circulating blood volume and decrease stress on the
○ The RAAS is activated in the kidney in response to low blood pressure, low intravascular volume, or low sodium levels. Renin is released by the kidney and converts to angiotensin I. Angiotensin I converts to angiotensin II in the lungs. Angiotensin II is a potent vasoconstrictor, resulting in systemic arterial vasoconstriction in an attempt to increase blood pressure. Angiotensin II also activates aldosterone from the adrenal glands, resulting in retention of sodium and water at the distal convoluted tubule of the kidney in an attempt to increase blood pressure. ● Heart rate is a major determinant of CO. Slow heart rates can result in less diastolic time and can result in poor ventricular filling. In addition, the coronary arteries fill during diastole. Fast heart rates can result in decreased coronary artery filling ■ Cardiac Output Monitoring - The CO is the amount of blood ejected by the heart each minute and is calculated from the heart rate and SV. Cardiac index (CI) is the CO adjusted for an individual’s size or body surface area. Monitoring of CO and CI is done to assess the heart’s ability to pump oxygenated blood to the tissues. Cardiac output is a measure of blood flow and is considered a reliable parameter to determine whether interventions have been successful. Causes of low and high CO are outlined in Two methods are commonly used to evaluate CO via the PA catheter: thermodilution cardiac output (TdCO) and CCO Low Cardiac Output/Index ● Heart rate that is too fast or too slow, leading to inadequate ventricular filling ● Stroke volume reduction as a result of: ○ Decreased preload ■ Hemorrhage ■ Hypovolemia from diuresis, dehydration, etc. ■ Vasodilation ■ Fluid shifts (i.e., third- spacing) outside the intravascular space ○ Increased afterload ■ Vasoconstriction ■ Increased blood viscosity ○ Decreased contractility ■ Myocardial infarction or ischemia ■ Heart failure ■ Cardiomyopathy ■ Cardiogenic shock ■ Cardiac tamponade High Cardiac Output/Index ● Heart rate elevation secondary to: ○ Increased activity ○ Anemia
○ Metabolic demands ○ Adrenal disorders ○ Fever ○ Anxiety ● Stroke volume increase as a result of: ○ Increased preload ■ Fluid resuscitation ■ Alteration in ventricular compliance ○ Decreased afterload ■ Vasodilation in sepsis ■ Decreased blood viscosity (anemia) ■ Increased contractility ■ Hypermetabolic states ○ Medication therapy ■ Determining CI ● (CO)/(BSA) = CI ○ Normal = 2.2-4. ■ Cardiac Output Monitoring ● Thermodilution method ○ Computation constant-based on the size of the catheter, the temp, and the amount of dilutent being administered ○ Inject D5W within 4 sec, smooth and rapidly ○ Do not handle the barrel of the syringe ○ Do 3 CO measurements, then average them ● Continuous CO Catheter ○ Invasive ○ Non-invasive/impedance method ● PAOP or PCWP (1) ○ Preload of the left ventricle ■ Normal 6-12 mmHg ● We want it to be between 12-18 mmHg when they have a PA cath ○ We want them to be compensating – higher than 12 is good ○ Too high (>18) is bad because it will stretch too much (overdue the Frank-Starling law) ○ Measureed at the end of expiration ■ The wedge pressure is measured by inflating the PA cath cuff inside of the capillary ● MUST be deflated or you risk pulmonary infarction ○ Necrosis r/t occlusion ○ When unable to wedge or not permitted to wedge the balloon for a PCWP/PAOP one may use the pulmonary artery diastolic pressure (PAD) ■ Normal is 4-12 mmHg
■ Obtain frequent blood samples for arterial blood gas analysis or other laboratory tests. ■ Can be used in conjunction with a stroke volume measurement device. ○ Arterial Pressure Measurements ■ MAP = [SBP + (2xDBP)]/ ● Must be >60 mmHg for vital organs to be perfused ■ Cuff BP is 5-20 mmHg lower than the direct Arterial BP ■ Arteries used: radial, brachial, femoral ○ Allen’s Test is performed ■ This is done before the insertion of the arterial line in the radial artery ● Also test before drawing ABGs from radial artery ■ Ask the patient to form a tight fist with the wrist in a neutral position. ● Occlude the radial artery by applying pressure with the thumb for approximately 10 seconds. ● Ask the patient to open fist while the clinician maintains thumb pressure on radial artery. ● Ulnar circulation is adequate if blanching resolves within 5 seconds, inadequate if hand remains pale for more than 10 seconds. ■ Modified Allen Test ● Ask the patient to form a tight fist with the wrist in a neutral position. ● Occlude radial and ulnar arteries for approximately 10 seconds. ● Ask patient to open fist, revealing a blanched hand. ● Release pressure on ulnar artery, maintaining pressure on radial artery. ● Ulnar circulation is adequate if blanching resolves within 5 seconds, inadequate if hand remains pale for more than 10 seconds. ○ Arterial Waveform ■ Systole ■ Dicrotic notch on arterial waveform represents closure of aortic valve ■ Diastole ■ NL MAP 70- ■ Damped waveform: ● Catheter lodged against the vessel wall ● Clot formation at the tip of the catheter ● Air in the transducer ● Kinks in the tubing system ● Make sure the patient is not becoming acutely hypotensive!!! ○ RN can remove arterial line ■ Apply pressure for 5-15 minutes ■ Femoral must press harder and longer ○ Indications for Arterial Pressure Measurements ■ For hemodynamically unstable patients for a continuous read out of SBP, DBP, & MAP ■ For frequent blood draws or ABGs ■ For patients in hypertensive crisis ■ Patients whose condition results in severe vasoconstriction or vasodilation ■ Ex: pt on a Nipride drip, Dopamine drip, ventilator ○ Complications of Arterial Pressure Monitoring ■ Thrombosis: may occur if a continuous flush solution is not used properly ● Prevent by keeping bag pumped to 300 ○ Must also check this pressure if bleeding from insertion site
■ Embolism: may occur as a result of small clot formation around the tip of the catheter or from air entering the system (air embolism) ■ ***Blood loss: result from sudden dislodgment of the catheter from the artery or from a disconnection in the tubing ■ Infection: May occur if the cath is left in place for a prolonged period, or a cut- down approach is used to insert the cath. *■ Numbness or tingling - not getting enough perfusion ○ Pulse Contour Cardiac Output Monitoring ■ A special device connected to the A-line that gives you CO, CI, PAOP, CVP ■ Aortic insufficiency, IABP, & PVD can’t be used to give accurate measurements ■ Less invasvive than PAL, yet can give you all the information of the PAL ■ In order to get accurate results the patient must be on a volume controlled ventilator ● Pulmonary Artery Catheter (3) ○ Allows us to indirectly measure information regarding Left Ventricular Function ○ Catheters - various types ○ Placement: ■ Catheter advanced to right atrium ■ Balloon is inflated ■ Pressure is low, usually 2-5 mmHg ■ Catheter is floated to right ventricle with the balloon inflated ■ Waveforms indicate a systolic pressure of 25-30 mmHg and a diastolic pressure of 0-5 mmHg ■ As the catheter moves into the pulmonary artery, the systolic pressure remains the same but the diastolic pressure elevates to 10-15 mmHg ■ The balloon is deflated and the catheter is moved until it can be wedged in a smaller vessel. ● Allow the balloon to passively deflate ○ If you must pull back - no more than 1.5 cc! ■ When the balloon is inflated the pressure recorded is that pressure in front of the catheter. It is an approximate measure of the left ventricular end diastolic pressure. ○ Pulmonary Artery Pressure Monitoring - Pulmonary artery catheters are used to diagnose and manage a variety of conditions in critically ill patients. The ability to measure pressures in the PA and the left side of the heart became reality after a flow- directed PA catheter was invented by doctors Jeremy Swan and William Ganz in 1970. Thermodilution PA catheters with ability to obtain PA pressures and CO measurement became the gold standard to which all new hemodynamic monitoring methods are compared. In the last 30 years, the PA catheter has been redesigned to obtain a variety of hemodynamic parameters, including measurements of continuous cardiac output (CCO), right ventricular end diastolic volume, right ventricular ejection fraction, and SvO ■ To determine pulmonary artery pressure (PAP), a specialized catheter is placed directly into the PA. The PA catheter is a long, flexible, multilumen, balloon- tipped catheter that enables measurement of several hemodynamic parameters. The proximal port lies in the right atrium and measures RAP; it is also used to administer fluids and medications and to obtain intermittent thermodilution CO measurements. The distal port measures PAP and PAOP; mixed venous blood samples are also drawn from this port. The thermistor port incorporates a
■ Air embolization ● Balloon rupture, poor technique during insertion, disconnected infusion line ■ Pulmonary thromboembolism ● Thrombus formation on the catheter d/t inadequate flushing ■ Pulmonary artery rupture ● Over inflation of the balloon, deflated balloon tip passes during insertion of the cath. causing perforations, frequent inflation of balloon ■ Pulmonary infarction ● Catheter movement into the wedged position, balloon left inflated, thrombus formation around the cath. Causing occlusion ○ You will see a wedge waveform on pulmonary catheter ○ Have pt cough, position on the left side ○ Implications for Use: ■ Assess left heart function with PAOP pressures. ■ Identify and treat cause of hemodynamic instability. ■ Assess pulmonary artery pressures. ■ Assess mixed venous oxygen saturation—SvO 2. ■ Directly measure cardiac output.
● Central Venous Catheter (CVC) (3) ○ Right Atrial Pressure/Central Venous Pressure Monitoring ■ In critically ill patients, the right atrial pressure (RAP) or CVP has been used to estimate central venous blood volume and right heart function. The pressure is obtained from the right atrial port of a pulmonary artery catheter (PAC) and is also called the RAP. Because no valves are present between the venae cavae and right atrium, both the CVP and RAP are essentially equal pressures. This measurement assesses preload of the right side of the heart. The term RAP is used most of the time in this textbook. Normal RAP/CVP ranges from 2 to 6 mm Hg. ■ The RAP is obtained from a central line inserted into the superior or inferior vena cava. The thoracic central veins (subclavian and internal jugular veins) are the most common insertion sites. Catheters used for RAP measurement are generally stiff and radiopaque, and they vary in length and diameter depending on the vein that is used. Shorter catheters are inserted into the subclavian and internal jugular veins, and longer catheters are used for insertion into the upper extremities or femoral vein. Central venous catheters often have multiple lumens that facilitate pressure monitoring, administration of fluids and medications, and blood sampling ○ Measures the CVP ■ Right atrial pressure ■ Reflects right ventricular end-diastolic pressure ■ Normal CVP is 2-8 mmHg ■ Usually measured via a central line: right internal jugular (RIJ) or right subclavian or left internal jugular (LIJ) or left subclavian or right and/or left femoral veins ■ If CVP is decreased it suggests dehydration ■ If CVP is elevated it suggests fluid excess, right ventricular failure, pulmonary artery HTN ■ Central Venous cath. Can be single, double, triple or quad lumen central line ■ Always use the distal port to hook it up for CVP readings ■ Look on the port to read distal port ■ Left atrial pressure : rarely measured, may measure in post CABG patient ○ Must get chest x-ray after placement ■ Especially with subclavian bc it can puncture the lung and cause a pneumo ■ For a femoral you just draw blood back to check placement ○ To measure anything you must use the distal port ○ CVC is a risk factor for a PE ○ Indications for Use: ■ Measure right heart filling pressures. ■ Estimate fluid status. ■ Guide volume resuscitation. ■ Assess central venous oxygen saturation—ScvO 2. ■ Administer large-volume fluid resuscitation or medications. ■ Access to place transvenous pacemaker. ● Intra-Aortic Balloon Pump (IABP) ○ Indications: *■ Cardiogenic shock, Unable to wean a pt from cardiopulmonary bypass machine, MI’s esp those who develop septal defect and are awaiting surgical
myocytes). This stimulates atrial contraction, however whenever the electrical impulse reaches the Purkinje fibers, this triggers ventricular contraction. ○ ECG- the electrical activity of normal conduction occurs downward between the left arm and the left leg (mean cardiac vector) or direction of current flow ■ Normal ECG tracing is composed of P, Q, R, S, & T waves. These waveforms arise from a flat baseline called the isoelectric line ■ P wave - represents atrial depolarization. Upright in leads 1 & 2. Normally, a P wave indicates that the SA node initiated the impulse that depolarized the atrium. A change in the shape of the P wave may indicate that the impulse arose from a site other than the SA node ■ PR interval - the downslope of the P wave returns to the isoelectric line for a short time before beginning the QRS complex. The interval from beginning of the P wave to the next deflection from the baseline is called the PR interval. This measures the time it takes for the impulse to depolarize the atria, travel to the AV node, and then enter the bundle of His. NORMAL PR interval is 0.12- 0.20 seconds (3-5 small boxes wide). When the PR interval is longer than normal, the speed of conduction is delayed to the AV node, when the PR interval is shorter than normal, the speed of conduction is abnormally fast ■ QRS complex - represents ventricular depolarization. Atrial repolarization also occurs simultaneously to ventricular depolarization. The classic QRS complex begins with a negative, or downward deflection immediately after the PR interval. The first negative deflection after the P wave is called the Q wave. If the first deflection from the isoelectric line is positive, or upright, the waveform is called an R wave. The S wave is a negative waveform that follows the R wave. It deflects below the isoelectric line. ■ QRS interval - is measured from where it leaves the isoelectric line of the PR interval to the end of the QRS complex. NORMAL QRS complex width is 0.06- 0.10 (1.5-2.5 small boxes). A QRS width greater than 0.10 may signify a delay in conduction through the ventricles (potentially caused by MI, atherosclerosis, cardiomyopathy) ■ T wave - represents ventricular repolarization. Generally no higher than 5 small boxes. Changes in T wave amplitude or direction can indicate electrical disturbances resulting from an electrolyte imbalance, or MI or injury. Ex: hyperkalemia causes tall peaked T waves, and ischemia may cause an inverted or up-side down T wave ■ ST segment - (plateau) connects the QRS complex to the T wave and is usually flat. The point at which the QRS complex ends and the ST segment begins is called the Junction point ■ QT interval - measured from the beginning of the QRS complex to the end of the T wave. This interval measures the total time taken for ventricular depolarization and repolarization. ABNORMAL PROLONGATION OF QT INTERVAL INCREASES VULNERABILITY TO LETHAL DYSRHYTHMIAS (VT and Vfib). Normally the QT interval becomes longer with slower heart rates and shorter with faster heart rates ■ U wave - if present, this waveform follows the T wave, it represents repolarization of a small segment of the ventricles. Larger U waves can be present in hypokalemia, cardiomyopathy, and digoxin toxicity. ○ Rate - represents how fast the heart is depolarizing. P waves are used to calculate the atrial rate, QRS waves are used to calculate the ventricular rate
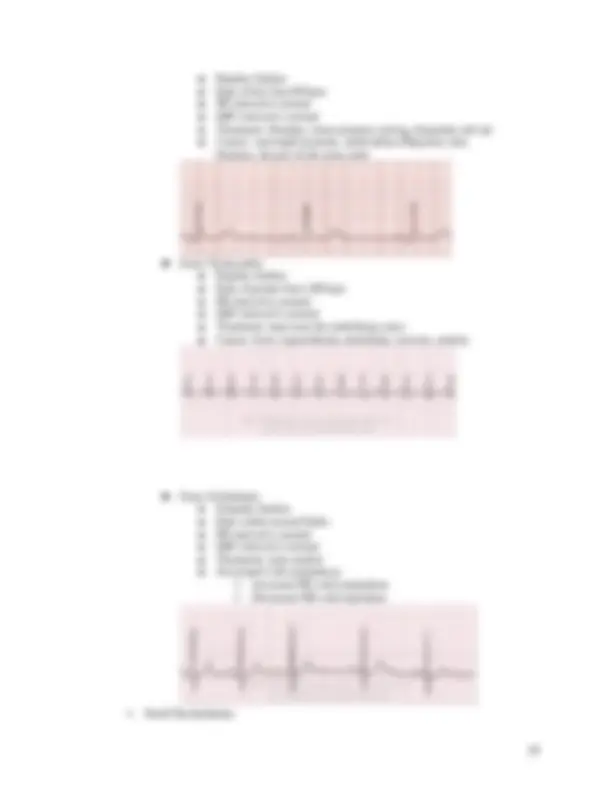
■ 6 second method- a quick & easy estimate of heart rate can be accomplished by counting the number of P waves or QRS waves within a 6 second strip to obtain atrial & ventricular heart rates per minute ○ Regularity - is assessed by using electronic or physical calipers, or a piece of paper & pencil. To determine atrial regularity, identify the P wave and place one caliper point on the peak of the P wave. Locate the next P wave and place the second caliper point on its peak. The second point is left stationary, and the calipers are flipped over. If the first caliper point lands exactly on the next P wave, the atrial rhythm is perfectly regular. If the point lands one small box or less away from the next P wave, the rhythm is essentially regular. If the point lands more than one small box away, the rhythm is considered irregular. Electronic calipers on some monitoring systems are used the same way ○ Measurement of PR, QRS, & QT/QTc intervals - measured and documented as part of rhythm analysis. PR intervals can change with dysrhythmias. QRS intervals can lengthen in response to new bundle branch blocks or with ventricular dysrhythmias. QT intervals can lengthen in response to certain drugs as well as electrolyte imbalances ○ ** Once an abnormal heart rhythm is identified, the priority is to assess the patient for any symptoms that may be related to the dysrhythmia. Assessing vital signs, LOC, lung sounds, asking if pt has chest pain or dyspnea, and obtain a 12 lead EKG. The next step is to determine if there are causes of the dysrhythmia that can be treated immediately ■ Ex: Patient with a fast, wide complex tachycardia who has a pulse but low blood pressure. The immediate priority is to treat the patient’s fast heart rhythm with a therapy such as emergent cardioversion, but the next critical step is to identify potential causes of the dysrhythmia, such as hypokalemia, hypomagnesemia, hypoxemia, or ischemia ○ Normal Sinus Rhythm - reflects normal conduction of the sinus impulse through the atria & ventricles. Sinus rhythm is initiated by an impulse in the sinus node. The generated impulse propagates through the conductive fibers of the atria, reaches the AV node where there is a slight pause, and then spreads throughout the ventricles, causing depolarization and resultant cardiac contraction in a timely and organized manner ■ Rhythm Analysis: ● Rate - Atrial & ventricular rates are the same & range from 60-100 bpm ● Regularity - Rhythm is regular or essentially regular ● Interval Measurements - PR interval is 0.12-0.20 second. QRS interval is 0.06-0.10 second ● Shape & sequence - P & QRS waves are consistent in shape. P waves are small and rounded. A P wave precedes every QRS complex, which is followed by a T wave ● Hemodynamic effect - patient is hemodynamically stable
● Care and treatment: The dysrhythmia itself is not treated, but the cause is identified and treated appropriately. For example, pain medications are administered to treat pain or antipyretics are given to treat fever. ○ Sinus Arrhythmia (1) ■ Sinus arrhythmia is a cyclical change in heart rate that is associated with respiration. The heart rate slightly increases during inspiration and slightly slows during exhalation because of changes in vagal tone. The ECG tracing demonstrates an alternating pattern of faster and slower heart rate that changes with the respiratory cycle ■ Rhythm Analysis ● Rate: Atrial and ventricular rates are between 60 and 100 beats/min. ● Regularity: This rhythm is cyclically irregular, slowing with exhalation and increasing with inspiration. ● Interval measurements: Measurements are normal. ● Shape and sequence: P and QRS waves are consistent in shape. P waves are small and rounded. A P wave precedes every QRS complex, which is then followed by a T wave. ● Patient response: This rhythm is tolerated well. ● Care and treatment: No treatment is required.
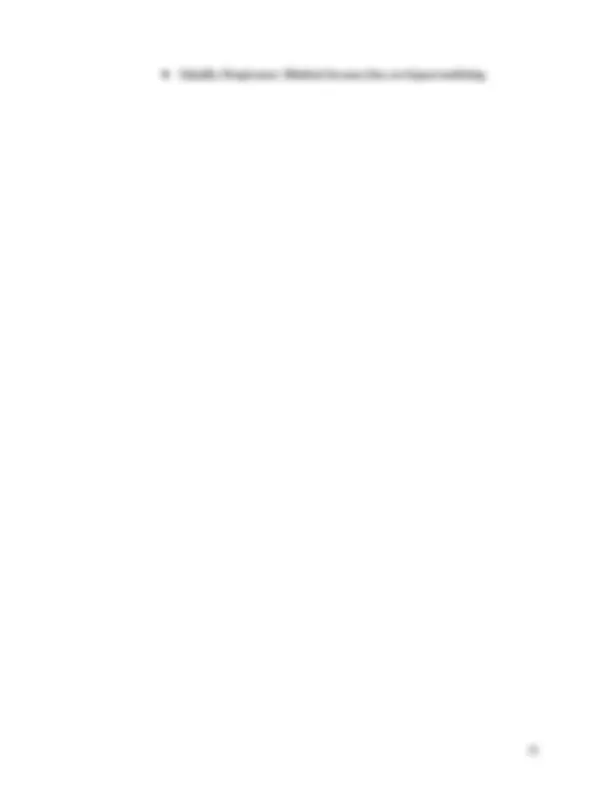
○ Sinus Bradycardia ■ Bradycardia is defined as a heart rate less than 60 beats/min. Sinus bradycardia may be a normal heart rhythm for some individuals such as athletes, or it may occur during sleep. Although sinus bradycardia may be asymptomatic, it may cause instability in some individuals if it results in a decrease in cardiac output. The key is to assess the patient and determine if the bradycardia is accompanied by signs of instability ■ Rhythm Analysis ● Rate: Both atrial and ventricular rates are less than 60 beats/min. ● Regularity: Rhythm is regular or essentially regular. ● Interval measurements: Measurements are normal, but QT may be prolonged. ● Shape and sequence: P and QRS waves are consistent in shape. P waves are small and rounded. A P wave precedes every QRS complex, which is followed by a T wave. ● Patient response: The slowed heart rhythm may cause a decrease in cardiac output, resulting in hypotension and decreased organ perfusion. ● Causes: Vasovagal response; medications such as digoxin or AV nodal blocking agents, including calcium channel blockers and beta blockers; myocardial infarction; normal physiologic variant in the athlete; disease of the sinus node; increased intracranial pressure; hypoxemia; and hypothermia may cause sinus bradycardia. ● Care and treatment: Assess for hemodynamic instability related to the bradycardia. If the patient is symptomatic, interventions include administration of atropine. If atropine is not effective in increasing heart rate, then transcutaneous pacing, dopamine infusion, or epinephrine infusion may be administered. Atropine is avoided for treatment of bradycardia associated with hypothermia. ○ Sinus Pauses ■ Sinus pauses occur when the SA node either fails to generate an impulse (sinus arrest) or the impulse is blocked and does not exit from the SA node (sinus exit block). The result of the sinus node not firing is a pause without any electrical activity ○ Sinus Arrest ■ Failure of the SA node to generate an impulse is called sinus arrest. The arrest results from a lack of stimulus from the SA node. The sinus beat following the arrest is not on time because the sinus node has been reset and the next sinus