Download Dermatology Revision Notes and more Study Guides, Projects, Research Clinical Medicine in PDF only on Docsity!
Dermatology Revision Notes BA/MBBS
Clinical Year Dermatology
Basic Principles
The skin functions as a barrier – made of the dermis and epidermis: The epidermis can be split into 4 main layers:
- Stratum corneum – composed of dead keratinocytes
- Stratum granulosum – has granules in keratinocytes
- Stratum spinosum – this layer is characterized by desmosomes between keratinocytes
- Stratum basalis – regenerative stem cell layer When taking an assessment of the skin, the history is very important. i) Nature of the problem
ii) Duration of the problem iii) Treatments so far iv) Allergies or Sensitivities:
- Including atopy (eczema, asthma, allergy) v) Sun exposure:
- Skin response to sun
- Can be classified by the Fitzpatrick skin type scale: Skin lesions can be classified into many different categories. These depend on the size, texture, colour and whether the lesion is raised or flat.
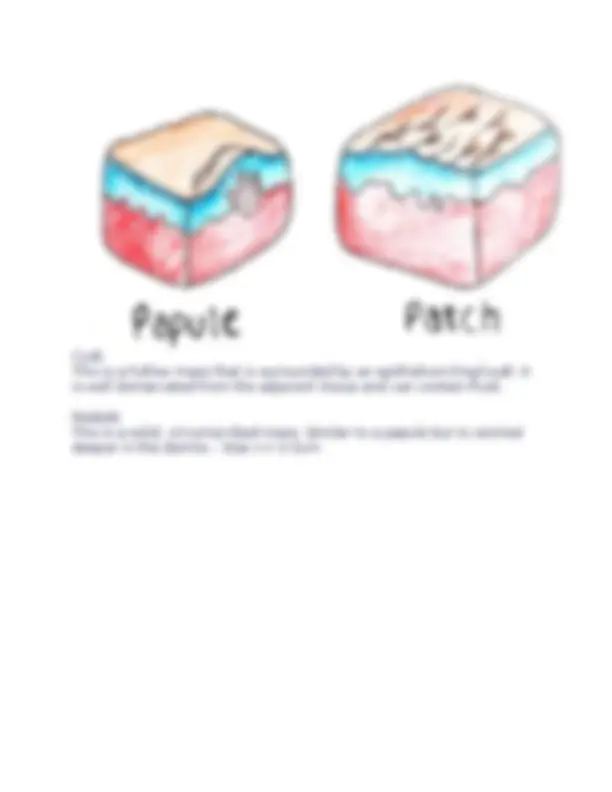
Macules –> Patches
These are flat, impalpable areas of skin without elevation or depression, but which does have a change in surface colour. They do not have any textural difference from the surrounding skin.
- Macule = <0.5cm
- Patch = >0.5cm
Cyst
This is a hollow mass that is surrounded by an epithelium-lined wall. It is well demarcated from the adjacent tissue and can contain fluid.
Nodule
This is a solid, circumscribed mass. Similar to a papule but is centred deeper in the dermis – Size =< 0.5cm
Wheal
A rounded, flat, red plaque that typically disappears in 24 hours, which is part of the inflammatory response
- Characterized by dermal oedema due to histamine release e.g. urticarial rash
Pustules
These are full of pus and consist of necrotic inflammatory cells.
- They can be sterile or infected
Fissures ➔ Erosions ➔ Ulcers
These are lesions which differ by the depth by which they penetrate the different layers of the epidermis
- Fissure = crack through epidermis to dermis
- Erosion = partial loss of the epidermis
- Ulcers = full thickness loss of epidermis
Eczema
Eczema (Dermatitis)
This is the general term which describes a condition which causes general inflammation of the skin.
Atopic Eczema (Atopic dermatitis)
This is the most common type of eczema and most common inflammatory disease of early childhood
- It affects about 20% of children under 5 and 2% of adults
- It is an immunologically mediated inflammatory skin reaction, mediated by increased Th2 cells
- This promotes pathogen specific IgE antibodies (type I hypersensitivity) increasing eosinophils and mast cells
Risk Factors: a) Atopy – associated with a family history of atopic conditions
- Often get eczema first, then asthma and rhinitis b) Diet – exacerbated in infants due to allergy to egg/cow’s milk protein Appearance:
- Erythematous, indistinct fissuring (cracks) through the epidermis
- For babies, lesions more concentrated around the face and the torso.
- As children get older, lesions are more likely to be found in the flexor surfaces (elbows, behind knees) and the creases of the face.
- This is because sweat concentrates here causing more irritation.
Management: i) Emollients
- These are liquids which are water based, aim to restore barrier function and flush our irritants
- Examples include Hydromol and Diprobase
- Prescribed in a ratio of 10:1 with a topical corticosteroid ii) Topical steroids – 1 fingertip unit (FTU) = 0.5g treats area twice that of human adult hand: Hydrocortisone (Mild strength) Eumovate (moderate) – a corticosteroid called clobetasone
Seborrheic eczema/dermatitis
This is a common, chronic type of dermatitis that primarily affects parts of the body which are rich in sebum, such as the scalp and face.
- It is thought to be due to an abnormal response to the fungus Malassezia furfur, which can lead to inflammation in the skin.
- It can affect both infants and adults giving rise to various symptoms.
i) Infants –> Usually seen in small children younger than 3 months
- It classically gives lesions with a yellowish-scale on the scalp (cradle- cap)
- Also affects axilla and groin areas giving a pink patchy rash which is not very itchy, so the baby is likely not to be perturbed by the rash. Management
- Regular washing with shampoo to clear scales
- If more severe, topical antifungal cream (ketoconazole) ii) Adults –> This usually starts in the late teens but is also seen in the elderly.
- Affects sebum rich areas (scalp, nasolabial areas, periorbital, behind ears)
- Gives pink thin scaly plaques in the folds which improve in summer (not itchy)
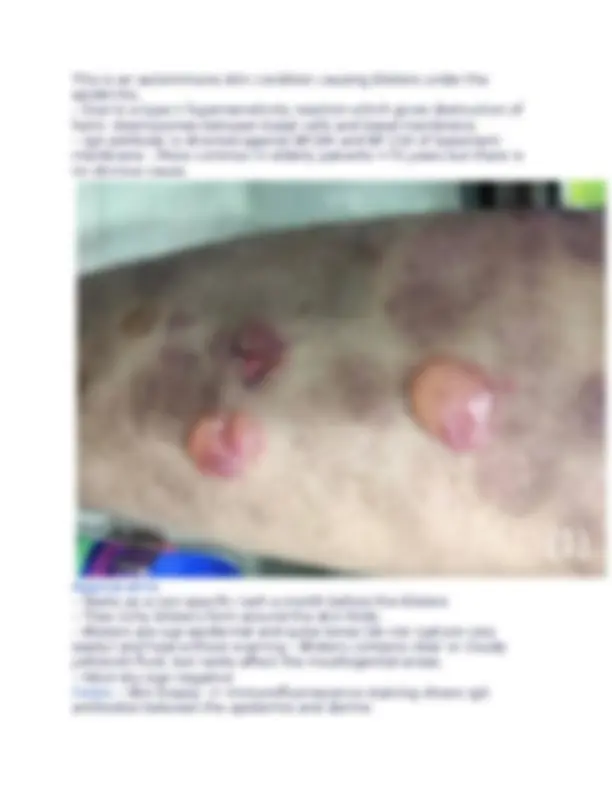
Appearance
- Leads to extensive crusted papules, and blisters, which can bleed
- Can be filled with clear yellow fluid or pus-like matter
- Swollen lymph glands and fever
- If untreated can start to affect the eyes, brain and lungs Diagnosis
- Clinical diagnosis (if doubt take swab and do PCR sequencing of viral DNA) Management
- A dermatological emergency –> Admit to hospital + Acyclovir
- If there is eye involvement, refer to ophthalmology
Contact dermatitis
This refers to inflammation of the skin which occurs due to direct contact with an agent, leading to redness, dryness and fissuring.
- It is the most common occupational skin disorder, and seen in populations of cleaners, food workers and hairdressers (wearing gloves).
Appearance
- Often seen on the hands due to direct contact (glove distribution)
- Erythema and itchiness, with drying/flaking of the skin
- Gives thickened skin with swelling, but crusting/vesicles are rare Management
- Improve hand routine –> Avoid soap, wear better gloves
- Can prescribe topical steroids and ensure frequent emollient use.
Dyshidrotic Eczema (Pompholyx)
This condition is characterized by blisters on the fingers, palms and soles of feet
- No known cause but related to seasonal allergies and stress and seen in adults Symptoms
- Starts as intense itching and burning of the skin on hands and fingers
- Forms large painful blisters which flake off
- Lasts up to 3 weeks before they dry off and heal
Scales and Flakes
This is excess shedding of the epidermis.
- e.g. Ichthyosis –> A rare genetic condition making dry, thickened, scaly skin
Crusting
This is when serous fluid or blood leaks under the skin and dries out. It can contain bacterial debris How to Describe Skin Lesions When describing skin lesions, we have to refer to 7 things to give a complete description. Remember by the 7S’s:
- Site
- Site on the body
- Distribution relative to each other
- Shade
- Pigmented
- Erythematous
- Yellow/orange
- Purpuric
- Style
- Size
- Shape
- Horizontal (outline)
- Vertical (cross-section)
- Annular
- Surface
- Smooth or rough
- Scaly/flaky
- Dry or moist
- Sides
- Well defined or indistinct
Inflammatory Dermatological Conditions
Acne Rosacea
This is a chronic skin disease of unknown cause in adults which characteristically affects the nose, cheeks and forehead, most often between the ages of 30-60.
- It is more common in white people with blue eyes, made worse by sunlight