


Elimination Disorders
•Introduction
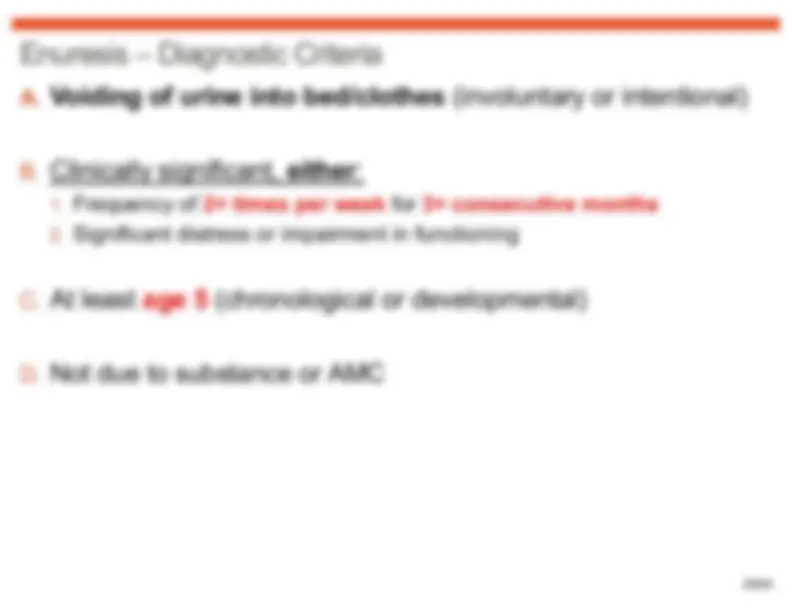
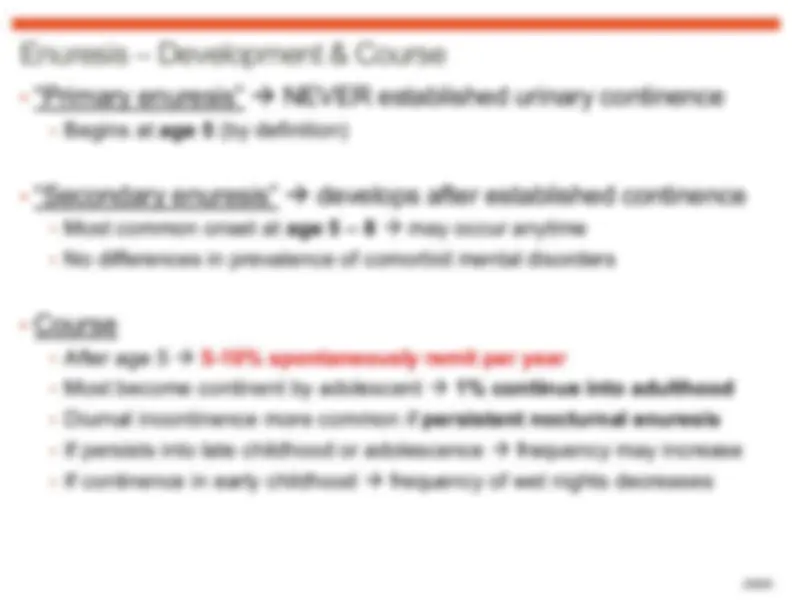
•Enuresis
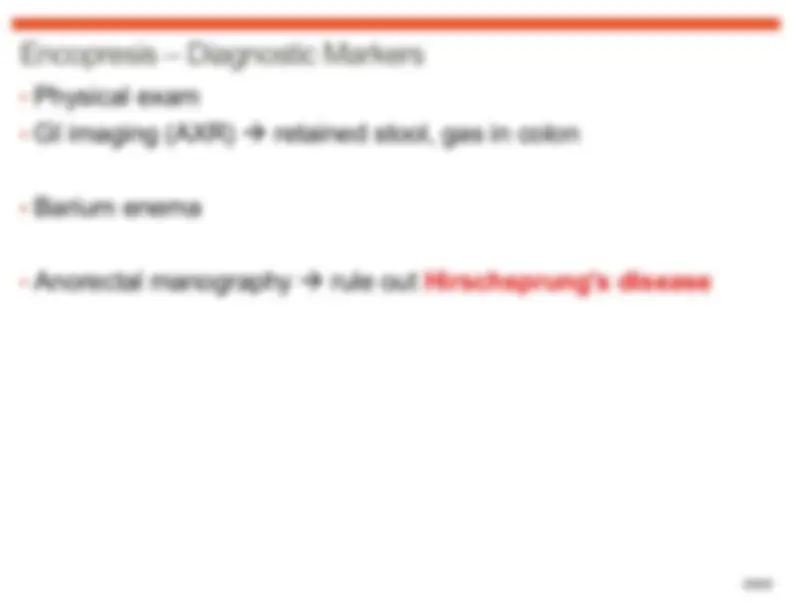
•Encopresis
•Other Specified Elimination Disorder
•Unspecified Elimination Disorder
Edits: L Jia 2021
Slides: B Chow

















Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
An overview of Elimination Disorders, focusing on Enuresis and Encopresis. It covers diagnostic criteria, subtypes, associated features, prevalence, development, risk factors, cultural and gender-related issues, functional consequences, differential diagnosis, comorbidity, and diagnostic markers. These disorders are characterized by the inappropriate elimination of urine or feces and typically first diagnosed in childhood or adolescence.
Typology: Lecture notes
1 / 30

This page cannot be seen from the preview
Don't miss anything!