Download envEnvironmental Factors effecting Toxicity Environmental Factors • Environmental modifyin and more Study notes Calculus in PDF only on Docsity!
Environmental Toxicology Unit 1
Toxicology
▪ The traditional definition of toxicology is "the science of poisons." ▪ As our understanding of how various agents can cause harm to humans and other organisms, a more descriptive definition of toxicology is " the study of the adverse effects of chemicals or physical agents on living organisms".
Historical Development
▪ The historical development of toxicology began with early cave dwellers who recognized poisonous plants and animals and used their extracts for hunting or in warfare. ▪ By 1500 BC, written recordings indicated that hemlock, opium, arrow poisons, and certain metals were used to poison enemies or for state executions. ▪ With time, poisons became widely used and with great sophistication. Notable poisoning victims include Socrates, Cleopatra, and Claudius. By the time of the Renaissance and Age of Enlightenment, certain concepts fundamental to toxicology began to take shape. The studies of Paracelsus (~1500AD) and Orfila (~1800 AD) are well known. ▪ In Ancient time (1500 BC) earliest collection of medical records contains many references and recipes for poisons. ▪ Discords (50 AD) a Greek physician, classify poisons as animal, plant or mineral & recognized the value of emetics Maimonides (1135-1204 AD), wrote about poisons and their antidote
Paracelsus a Swiss physician, alchemist
- Determined that specific chemicals were actually responsible for the toxicity of a plant or animal poison.
- He also documented that the body's response to those chemicals depended on the dose received.
- His studies revealed that small doses of a substance might be harmless or beneficial whereas larger doses could be toxic.
- This is now known as the dose-response relationship, a major concept of toxicology.
- Paracelsus was one of the founders of modern toxicology.
- His best known quote: All substances are poisons; it is the dose that makes the poison.
Orfila, a Spanish physician,
- is often referred to as the founder of toxicology.
- It was Orfila who first prepared a systematic correlation between the chemical and biological properties of poisons of the time.
- He demonstrated effects of poisons on specific organs by analyzing autopsy materials for poisons and their associated tissue damage.
- The 20th century is marked by an advanced level of understanding of toxicology.
- DNA (the molecule of life) and various biochemicals that maintain body functions were discovered.
- Our level of knowledge of toxic effects on organs and cells is now being revealed at the molecular level.
- It is recognized that virtually all toxic effects are caused by changes in specific cellular molecules and biochemicals
Xenobiotic is the general term that is used for a foreign substance taken into the body. It is
derived from the Greek term xeno which means "foreigner." Xenobiotics may produce beneficial effects (such as a pharmaceuticals) or they may be toxic (such as lead).
- Toxicity – is the ability of a chemical agent to cause injury. It is a qualitative term which depends on the amount of chemical absorbed, severity of the exposure, dose & others.
- It can be acute (toxic event which occurs soon after acute or limited exposure), or chronic (apply to an event which occurs many weeks, months or years after exposure). o Acute exposure is a single exposure – or multiple exposures occurring over 1 or 2 days. o Chronic exposure is multiple exposures continuing over a longer period of time
- Hazard – is the likelihood that injury will occur in a given situation or setting: the conditions of use and exposure are primary considerations.
- Risk – is defined as the expected frequency of the occurrence of an undesirable effect arising from exposure to a chemical or physical agent. Toxic substances may be systemic toxins or organ toxins.
- A systemic toxin is one that affects the entire body or many organs rather than a specific site. For example, potassium cyanide is a systemic toxicant in that it affects virtually every cell and organ in the body by interfering with the cell's ability to utilize oxygen.
- Organ Toxins: Toxicants may also affect only specific tissues or organs while not producing damage to the body as a whole. These specific sites are known as the target organs or target tissues. Some examples: Benzene is a specific organ toxin in that it is primarily toxic to the blood-forming tissues. Lead is also a specific organ toxin; however, it has three target organs (central nervous system, kidney, and hematopoietic system).
Toxic agent or substance
Based on the organ/system effect
- Cardiovascular toxicology
- Renal toxicology
- Central nervous system toxicology
- Gastrointestinal toxicology
- Pulmonary Toxicology 1. You need to prepare 1000 mL of a 10 ppm Cu²⁺ solution using CuSO₄·5H₂O (molar mass = 249.7 g/mol). How much salt should you weigh? 2. Prepare 500 mL of a 5 ppm Zn²⁺ solution using ZnCl₂ (molar mass = 136. g/mol). How many mg of ZnCl₂ will you dissolve?
3. To prepare 250 mL of a 20 ppm Fe³⁺ solution using Fe(NO₃)₃·9H₂O (molar mass = 403.9 g/mol), how much salt should be added? 4. You want to make 1 liter of a 1 ppm Pb²⁺ solution from Pb(NO₃)₂ (molar mass = 331.2 g/mol). What mass of Pb(NO₃)₂ is required? 5. Prepare 100 mL of a 1% (w/v) NiSO₄ solution. How many grams of NiSO₄ should you weigh? 6. You need 250 mL of a 0.5% (w/v) CuCl₂ solution. What mass of CuCl₂ should be added? Mercury spilled from a broken thermometer contaminated the lab bench. Toxicant Botulinum toxin, made by bacteria, can cause severe paralysis. Toxin
Toxicology: types and Dose EXPOSURE ROUTES
- It has been estimated that about 70,000 chemicals are used worldwide, and the chemical industry introduces about 200 to 1,000 new chemicals each year.
- Because of this, we are exposed to a number of chemicals in our home, at work, and in the general environment.
- Trace amounts of toxic chemicals are present in the food, the air, and the drinking water. Exposure to toxic substances occurs through the three major routes listed below Dermal Absorption:
- Contact with the skin is the most common path of toxic substance exposure
- The skin is composed of three layers:
- Epidermis (outer layer). The outermost layer is the stratum corneum (carnified layer). This is the structure that determines the rate of absorption of substances through the epidermis. For example, a pesticide such as Malathion(organophosphate insecticides), which easily penetrates the stratum corneum, moves quickly through the other layers of the skin and is rapidly absorbed into the bloodstream. DDT, another type of pesticide, does not easily penetrate the stratum corneum, so the rate of absorption is much slower.
- Dermis (inner layer ). The inner layer of the skin is sometimes referred to as the true skin. In animal hides, this is the layer that turns to leather when chemically processed. The dermis is the source of oxygen and of nutrients for the epidermis. The hair follicles, sweat glands, and sebaceous (oil) glands are found in this layer. These structures play a limited role in the absorption of substances across the skin.
- Subcutaneous fatty tissue. This layer provides a cushion for the underlying structures and allows the skin to move to some extent. Factors affecting dermal absorption of toxic substances include I. The condition of the skin. II. An intact stratum corneum (epiderms) is an effective barrier to absorption of some toxic chemicals. However, physical damage to the protective barrier, such as a cut or abrasion, allows toxic substances to penetrate the epidermis and enter the dermis where they more readily enter the bloodstream and are carried to other parts of the body. III. The chemical makeup of the substance. Inorganic chemicals and substances are not easily absorbed through intact, healthy skin (such as cadmium, lead, mercury, and chromium. Organic chemicals dissolved in water do not easily penetrate the skin because the skin is impermeable to water. However, organic solvents, such as paint thinner or gasoline, are easily absorbed through the epidermis.
IV. Increasing the concentration of the toxic substance or the exposure time can increase the rate or amount of material absorbed. INHALATION:
- Inhalation is the easiest and fastest means of exposure to toxic substances because toxic substances are readily absorbed in the respiratory tract.
- The lining of the respiratory tract is NOT effective in preventing absorption of toxic substances into the body.
- The respiratory tract consists of the nasal passages, trachea (windpipe), larynx (voice box) and the lungs.
- The following factors affect inhalation of toxic substances:
- Concentration of toxic substance in the air
- Solubility of substance in the blood and tissue,
- Respiration rate,
- Length of exposure,
- Condition of respiratory tract,
- Size of toxic particle. INGESTION
- Ingestion of toxic substances usually occurs accidentally or unknowingly.
- The digestive tract consists of the mouth, the esophagus (food canal), stomach, and intestine (large and small).
- The major function of the digestive tract is to digest and absorb the foods we eat. INJECTION
- Injections are another common route for exposure.
- Injections are mainly used in laboratory studies on experimental animals.
- Following are the different types of injections:
- Intravenous injections (into a vein).
- Intramuscular injections (into the muscle).
- Intra peritoneal injections (into the abdominal cavity).
- Intradermal injections (into the skin).
- Subcutaneous injections (under the skin). ELEMENTS FOR A PATHWAY OF EXPOSURE
- Elements for a Pathway of Exposure ATSDR (Agency for Toxic Substances and Diseases Registry) defines an exposure pathway as the process by which an individual is exposed to contaminants that originate from some source of contamination
- A potential exposure pathway exists when one or more of the elements is missing, but available Information indicates that exposure is likely.
- An incomplete exposure pathway exists when one or more of the elements is missing and available information indicates that exposure is not expected to occur.
- For exposure to occur, a completed exposure pathway must exist. A completed exposure pathway exists when all of the following five elements are present:
- A source of contamination , for example a smoke stack on a factory;
- Media for the contaminant to travel , such as groundwater, surface soil, surface water, air, subsurface soil, sediment, and biota (animal and plant life)
- Chronic, which is exposure to a chemical for more than 3 months.
- Sub-acute, which is exposure to a chemical for 1 month or less.
- Sub-chronic, which is exposure to a chemical between 1 to 3 months.
Effects and Exposure
- Local effects are seen at or near the body part or parts where exposure occurred.
- For example, inhaling particles can result in irritation of the respiratory tract, resulting in effects ranging from sneezing to chest pains and difficulty in breathing. An ant bite leads to redness and swelling at the bite location.
Types of Biologic Markers
The NRC (1987) classifies biomarkers into three main types:
1. Markers of Exposure
- Definition: Indicators that a chemical agent or its metabolite has entered and interacted with the body.
- Examples: o Blood lead levels (for lead exposure) o Urinary phenol (for benzene exposure) o DNA or protein adducts (for genotoxic chemicals)
- Represent internal dose and biologically effective dose in the continuum.
2. Markers of Effect
- Definition: Biochemical, physiological, or structural alterations signaling an early or ongoing response to exposure.
- These changes might not yet be disease but could predict disease development.
- Examples: o Elevated liver enzymes (after solvent exposure) o DNA damage or chromosomal aberrations o Altered hormone or immune function
- Represent the early biologic effect and altered structure/function parts of the continuum.
3. Markers of Susceptibility
- Definition: Indicators of inherent or acquired capacity to respond differently to a given exposure.
- Factors can be genetic , metabolic , or lifestyle-related.
- Examples:
o Genetic polymorphisms in detoxifying enzymes (e.g., GST, CYP450) o Immune status or nutritional deficiencies
- These markers affect risk at all stages —from exposure uptake to disease prognosis. Continuum from Exposure to Disease (Figure 7-1) Stage Biomarker Type Description Exposure → Internal Dose (ID) Exposure Marker Amount absorbed into the body Biologically Effective Dose (BED) Exposure Marker Amount interacting with target tissues Early Biologic Effect (EBE) Effect Marker Initial biological response Altered Structure/Function (ASF) Effect Marker Detectable precursor to disease Clinical Disease (CD) Disease Marker Observable, diagnosable illness Prognostic Significance (PS) Disease Marker Predicts disease outcome or progression Susceptibility Susceptibility Marker Modifies risk across all stages
Duration and Frequency of Exposure.
- There is a difference in type and severity of effects depending on how rapidly the dose is received (duration) and how often the dose is received (frequency).
- Acute exposures are usually single incidents of relatively short duration--a minute to a few days.
- Chronic exposures involve frequent doses at relatively low levels over a period of time ranging from months to years. I f a dose is administered slowly so that the rate of elimination or the rate of detoxification keeps pace with intake, it is possible that no toxic response will occur. The same dose could produce an effect with rapid administration.
Factors Influencing Toxicity
Type Examples Factors related to the chemical Composition (salt, free base, etc.); physical characteristics (particle size, liquid, solid, etc.); physical properties (volatility, solubility, etc.); presence of impurities; breakdown products; carrier. Factors related to exposure Dose; concentration; route of exposure (ingestion, skin absorption, injection, inhalation); duration; frequency. Factors related to the person exposed Heredity; immunology; nutrition; hormones; age; sex; health status; preexisting diseases. Factors related to environment Carrier (air, water, food, soil); additional chemicals present (synergism, antagonism, potentiation); temperature; pressure (air/barometric); other abiotic factors (e.g., pH, salinity, humidity).
- Toxic concentration low (TCLO): The lowest concentration of a substance in air to which humans or animals have been exposed for any given period of time that has produced any toxic effect in humans or produced tumorigenic or reproductive effects in animals
- Lethal dose low (LDLO): The lowest dose, other than LD50 of a substance introduced by any route, other than inhalation, which has been reported to have caused death in humans or animals. Category Exposure Time Route of Exposure Toxic Effects (Human) Toxic Effects (Animal)
TD ₗₒ Acute or
chronic All except inhalation Any nonlethal Reproductive, Tumorigenic
TC ₗₒ Acute or
chronic Inhalation Any nonlethal Reproductive, Tumorigenic
LD ₗₒ Acute or
chronic All except inhalation Death Death
LD₅₀ Acute^ All except
inhalation Not applicable Death (statistically determined)
LC ₗₒ Acute or
chronic Inhalation Death Death
LC₅₀ Acute^ Inhalation^ Not applicable^ Death (statistically
determined) The Dose makes it Poison MICRONUTRIENTS: Nutrient Sources RDA or AI (adults > 19 years) Vitamin B1 (thiamine) Whole grains, meat, fish 1.1–1.2 mg Vitamin B2 (riboflavin) Organ meats, eggs, milk 1.1–1.3 mg Vitamin B3 (niacin) Meat, salmon, leafy greens, beans 14 – 16 mg Vitamin B5 (pantothenic acid) Organ meats, mushrooms, tuna, avocado 5 mg
Vitamin B6 (pyridoxine) Fish, milk, carrots, potatoes 1.3 mg Vitamin B7 (biotin) Eggs, almonds, spinach, sweet potatoes 30 mcg Vitamin B9 (folate) Beef, liver, black-eyed peas, spinach, asparagus 400 mcg Vitamin B12 (cobalamin) Clams, fish, meat 2.4 mcg Vitamin C (ascorbic acid) Citrus fruits, bell peppers, Brussels sprouts 75 – 90 mg
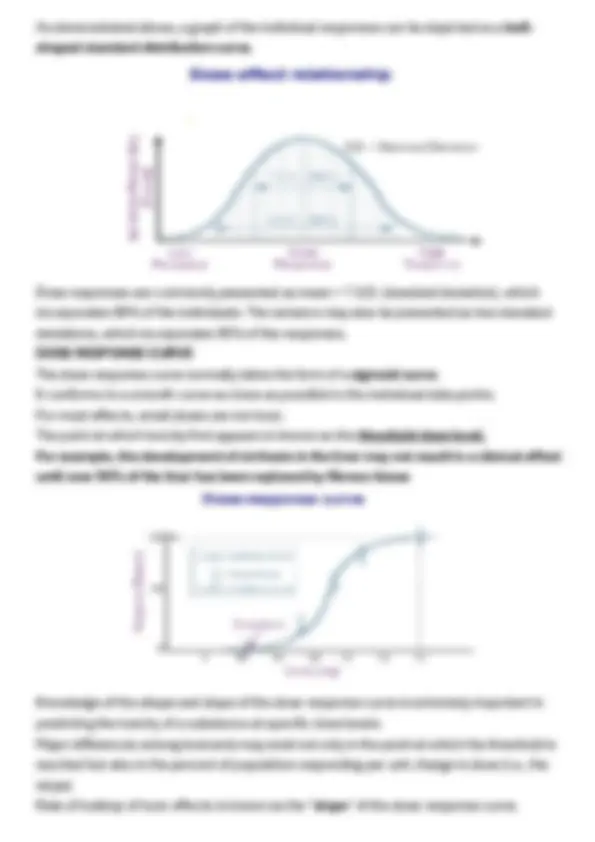
The Dose response Relationship (biologically effective dose)
- The dose-response relationship is a fundamental and essential concept in toxicology.
- It correlates exposures and the spectrum of induced effects.
- Generally, the higher the dose, the more severe the response.
- The dose-response relationship is based on observed data from experimental animal, human clinical, or cell studies. DOSE-EFFECT RELATIONSHIP Knowledge of the dose-response relationship: - establishes causality that the chemical has in fact induced
- the observed effects - establishes the lowest dose where an induced effect occurs
- the threshold effect - determines the rate at which injury builds up
- the slope for the dose response. Within a population, the majority of responses to a toxicant are similar; however, a wide variance of responses may be encountered, some individuals are susceptible and others resistant.
Calcium
Your body needs calcium to build and maintain strong bones. Your heart, muscles and nerves also need calcium to function properly. Hypercalcemia ( Too much calcium in the blood can weaken bones and create kidney stones.) There may be a link between high-dose calcium supplements and heart disease Calcium and prostate cancer. It also can affect the heart and brain
DOSE ESTIMATES
Dose-response curves are used to derive dose estimates of chemical substances. A common dose estimate for acute toxicity is the LD50 (Lethal Dose 50%). NOAEL and LOEAL Based on the actual data points from human clinical or experimental animal studies Two terms often encountered are No Observed Adverse Effect Level (NOAEL) Low Observed Adverse Effect Level (LOAEL). NOELs and LOELs do not necessarily imply toxic or harmful effects and may be used to describe beneficial effects of chemicals as well
APPLICATION OF DOSE RESPONSE REALTIONSHIP FOR COMPARISON
Different types of dose and response relationships a) Linear-no-threshold response b) Threshold response c) Hormetic or J-shaped response d) saturation curve, e) Sigmoid curve, f) U-shaped (continuous) and inverted U-shaped (dotted) curves. STATISTICAL MODELLING
- Statistical analysis of dose–response curves may be performed by regression methods such as the probit model or logit model
- Empirical models based on nonlinear regression are usually preferred over the use of some transformation of the data that linearizes the dose-response relationship
Hill’s Equation
- Logarithmic dose–response curves are generally sigmoidal and monotonic and can be fit to a classical Hill equation.