J. ANASTACIO│SECTION 14
Hypothalamic & Pituitary Function
Hypothalamic & Pituitary Function
INTRODUCTION
→ MASTER GLAND (pituitary)
→” To spit mucus” (Greek & Latin term)
→
Hypophysis (undergrowth)- due to its position under the
hypothalamus
→Was later proven to be signaled by the brain to secrete
hormones w/c regulate other endocrine glands
→ ABSENCE OF PITUITARY
• Cessation of growth
• Failure of G.T.A. (gonadal, thyroidal, & adrenal)
functions
→TRANSPONDER (transmitter & responder)
• Translates neural input into a hormonal product
• Main na nagrreceive ng signal then magttransmit ng
signal
• EXAMPLE: PG receives signal from the hypothalamus
then hormones will be secreted
→MEDIAN EMINENCE
• Inferior portion of the hypothalamus
• Together w/ pituitary stalk is critical event in the
formation of hypothalamic-hypophyseal unit
→ DIAPHRAGMA SELLA
• Reflection of dura
• Separates the superior portion of the pituitary from the
hypothalamus
• Penetrated by the infundibulum or pituitary stalk
→INFUNDIBULUM
• Connects the anterior pituitary (adenohypophysis) to
the M.E & hypothalamus
• Contains neural & vascular structures that terminate in
the hypophysis
→POSTERIOR PITUITARY
• Neurohypophysis
• Connected to the supraoptic & paraventricular
hypothalamic nuclei (where vasopressin & oxytocin are
produced) by 2 distinct neurosecretory tracts:
“supraopticohypophyseal & tuberohypophyseal”
→HYPOTHALAMIC-HYPOPHYSIAL PORTAL SYSTEM
• Contained in the infundibulum
• Where the adenohypophysis receives 80-90% of blood
supply & hypothalamic factors
• Primary plexus is in the M.E & is composed of capillaries
lacking a blood-brain barrier (fenestrated capillaries)
• Where hypothalamic nuclei that modulate pituitary
fxn terminate their axons
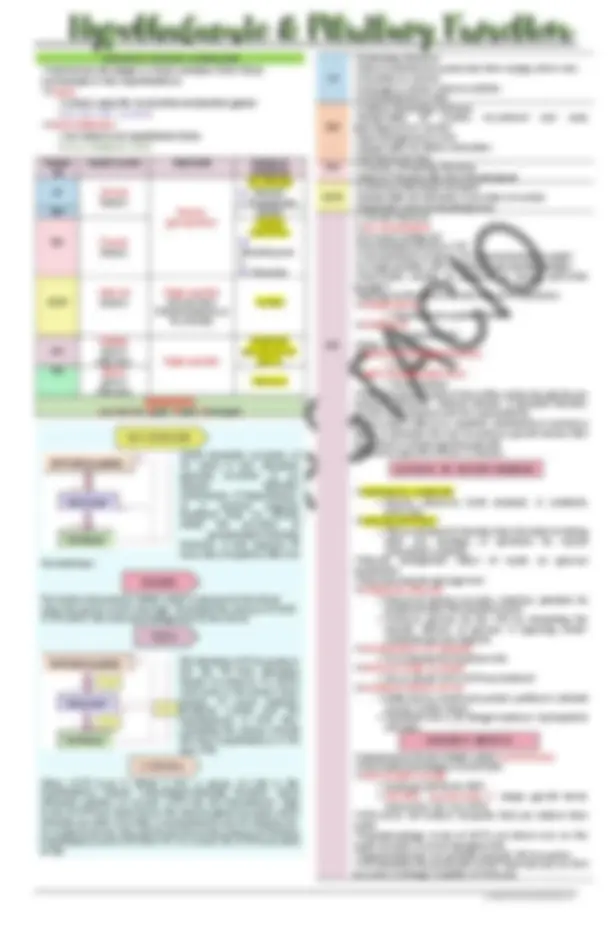
→LACTOTROPHS- Prolactin-secreting cells
→SOMATOTROPHS- Growth Hormone-secreting cells
→THYROTROPHS- Thyroid Stimulating Hormone-secreting cells
→CORTICOTROPHS- AdrenoCorticoTropin Hormone-secreting
cells
→GONADOTROPS-Luteinizing Hormone & Follicle Stimulating
Hormone-secreting cells
→Pulsatile secretions
→Feedback loops
→Environmental or External modification of
performance
→Diurnal rhythms
→OPTIC CHIASM is near the pituitary gland so if there’s a
pituitary tumor, the px will experience symptoms such as
disturbance in vision because the optic chiasm is being
pressed against it.
→HYPOTHALAMUS small region; links nervous system to
endocrine through the adenohypophysis (Anterior pituitary).
Then the adenohypophysis will secrete hormones that will
go to different endocrine glands.
OUTLINE
INTRODUCTION
HYPOTHALAMIC HORMONES
ANTERIOR PITUITARY HORMONES
POSTERIOR PITUITARY HORMONES
HORMONE SECRETION ABNORMALITIES
HYPOPITUITARISM
Hypothalamus
synthesizes
oxytocin,
arginine
vasopressin
(AVP), adh, etc
Hypothalamus
stimulates
release
Hormones
Release
hormones to
Luh Punta Si GandHang Tita Tomorrow Sa Hauz Coz Ang
Cute Tignan ng Hauz Gusto Lang pala Humingi Free
Sample ng Hotdog
Hormones released
by hypothalamus
are releasing
hormones
ANTERIOR PITUITARY CELL TYPES
FUNCTIONS
Patrick Fed Eli Doritos
Vasopressin &
oxytocin are
produced in the
hypothalamus
(Adenohypophysis)
(Neurohypophysis)
(Infundibulum)
LOCATION: base of the brain & above
the pituitary; connected to PPG
through infundibulum