Partial preview of the text
Download Intracranial pressure and more Summaries Nursing in PDF only on Docsity!
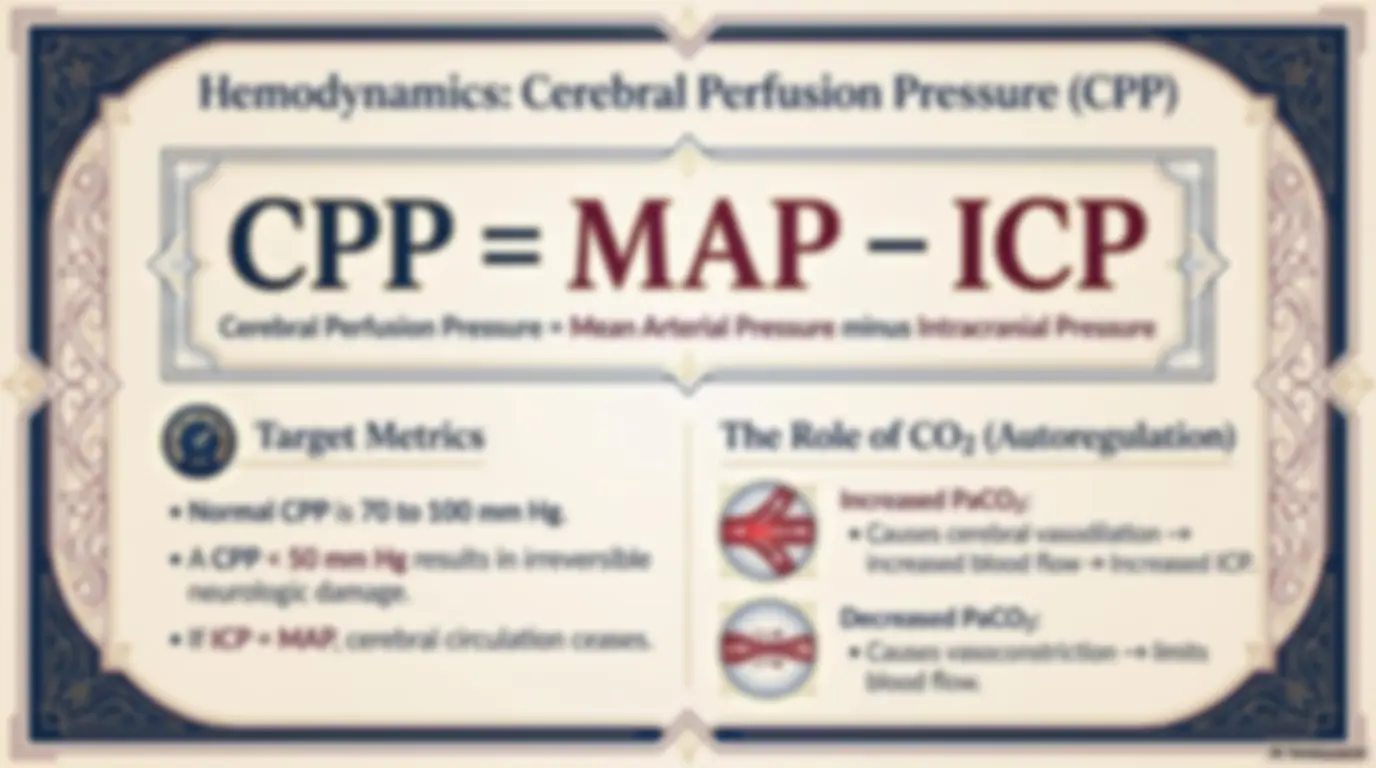
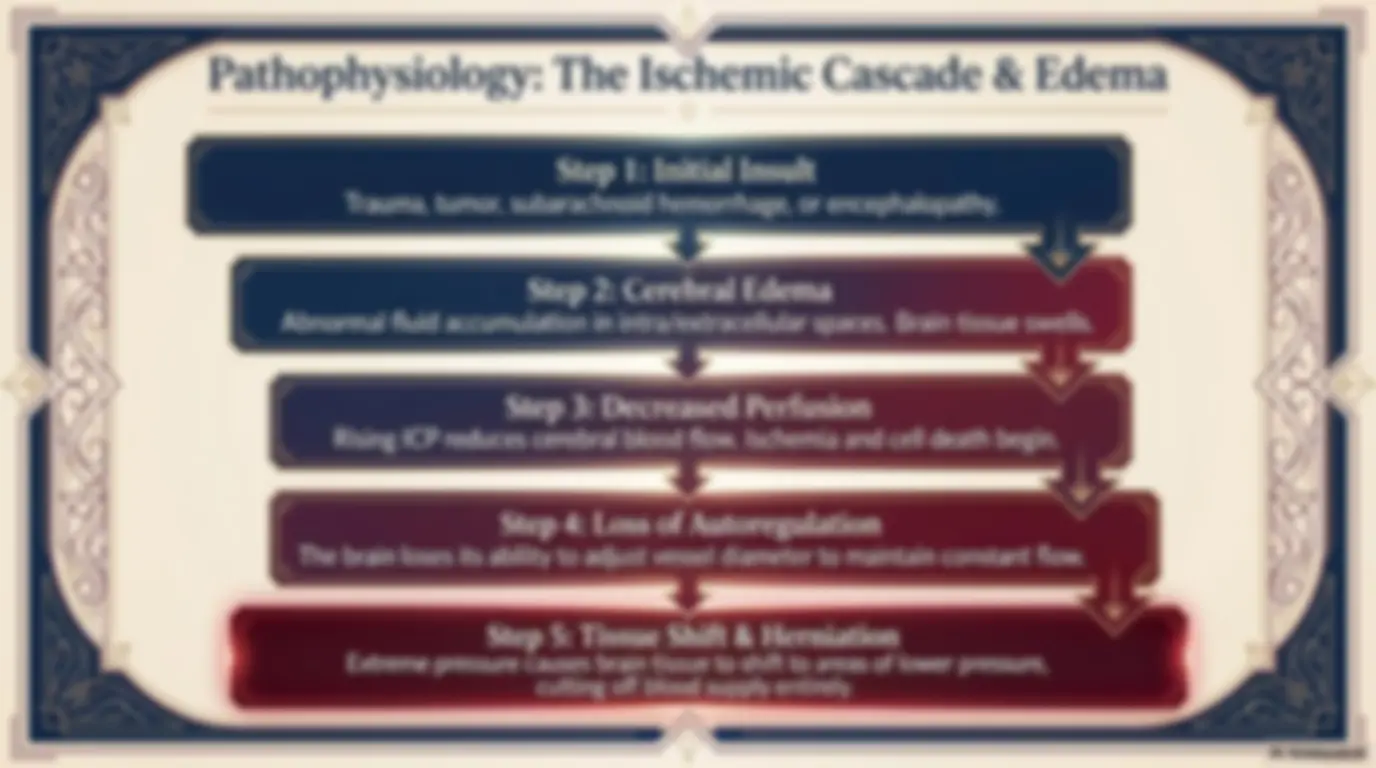
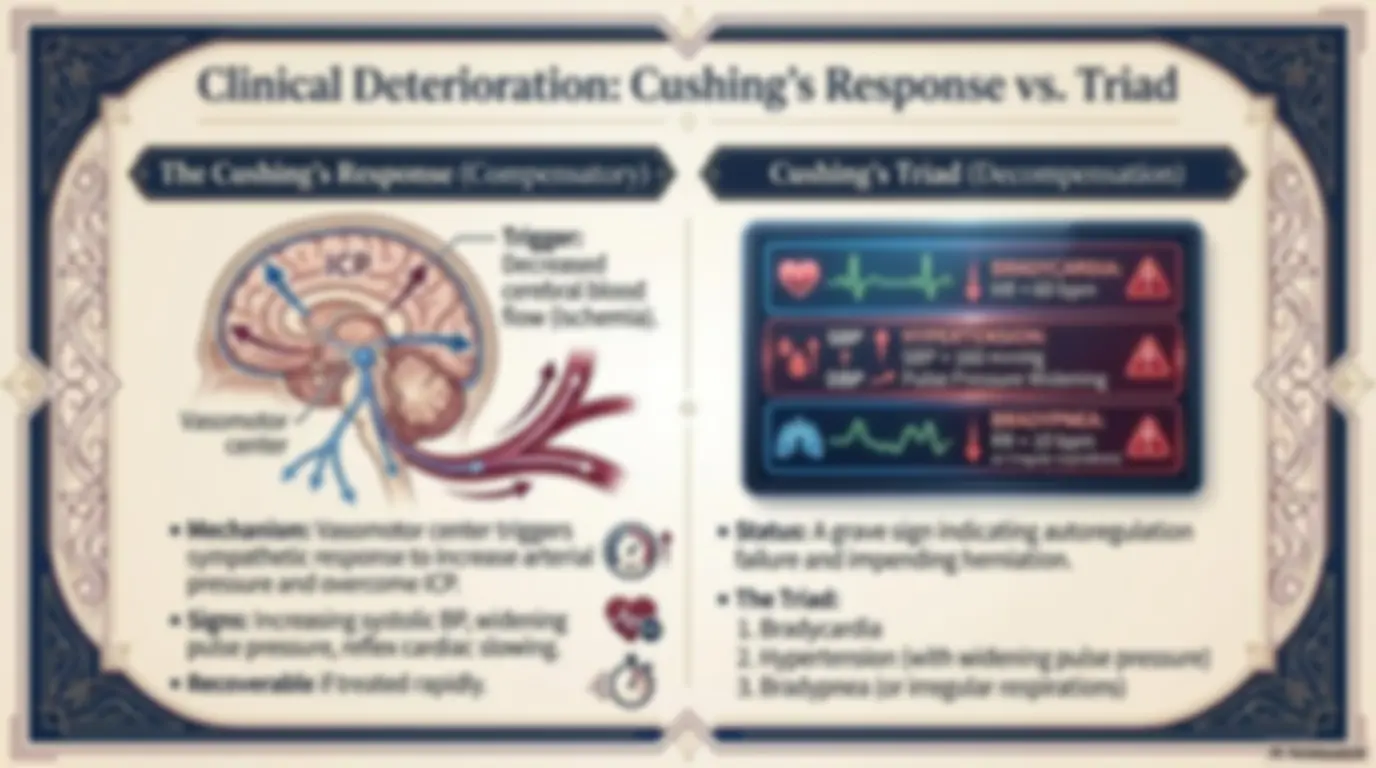
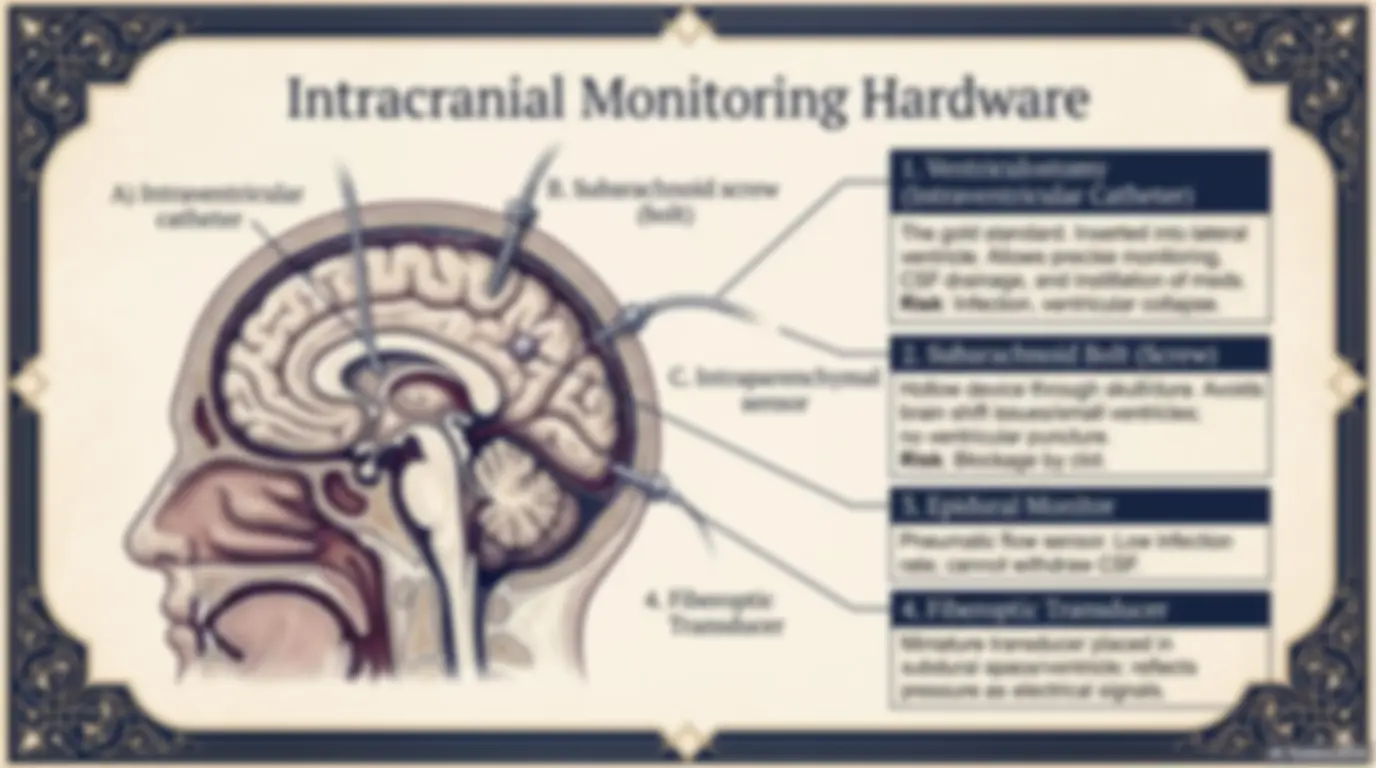
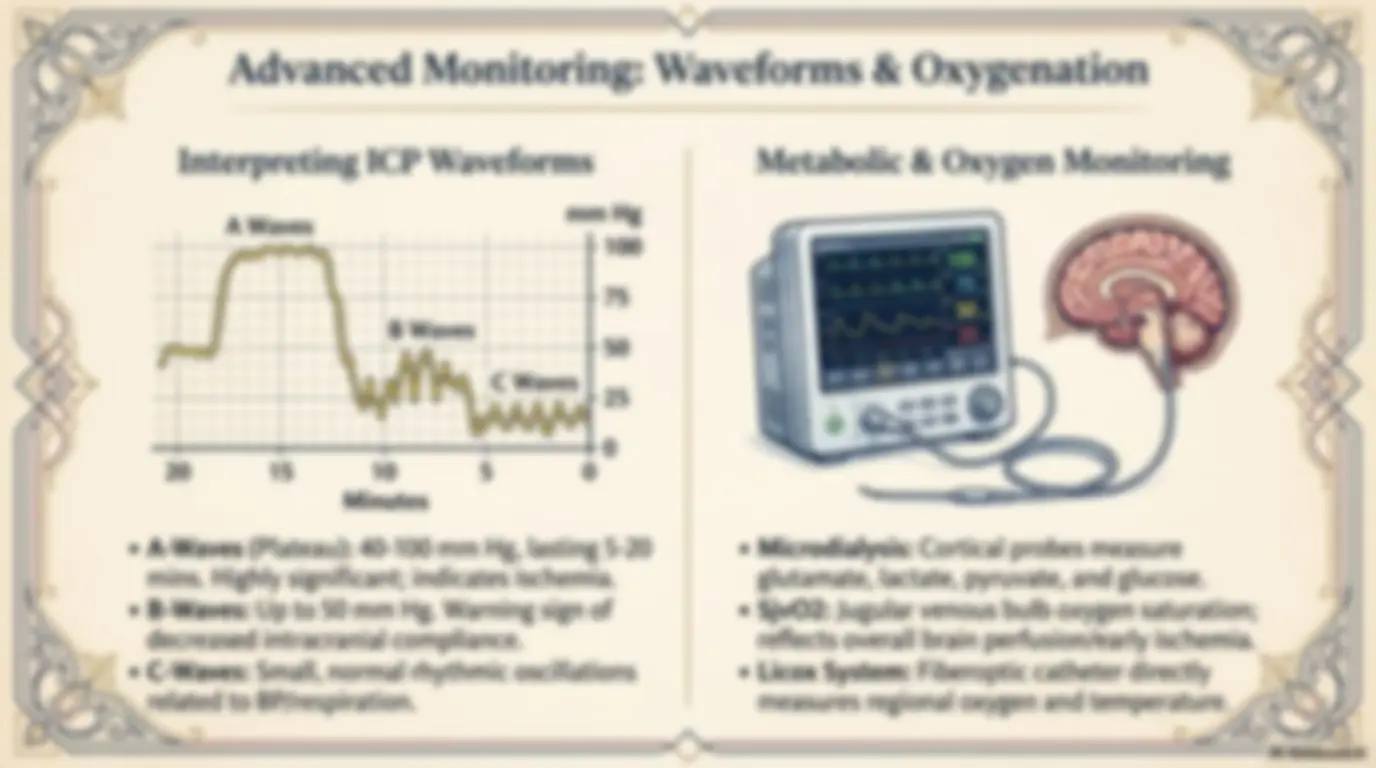
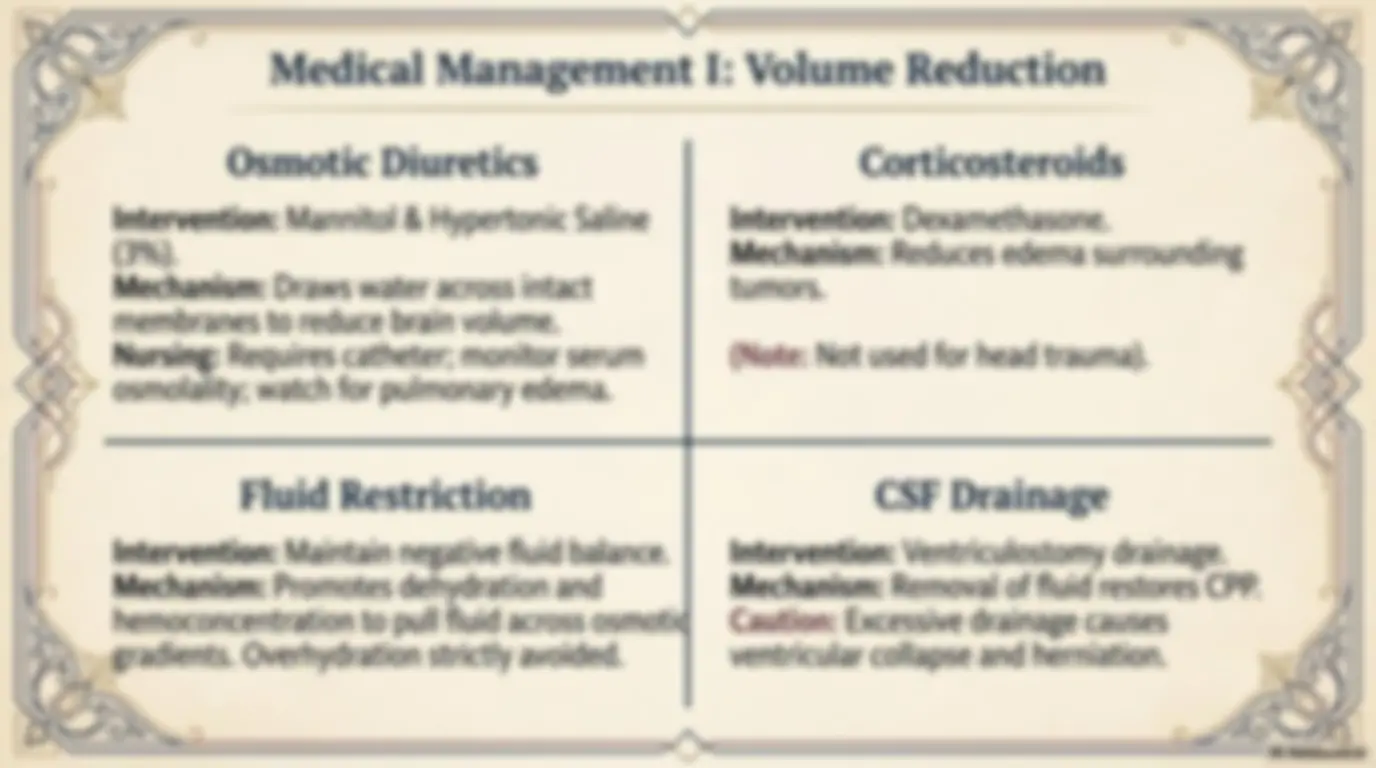
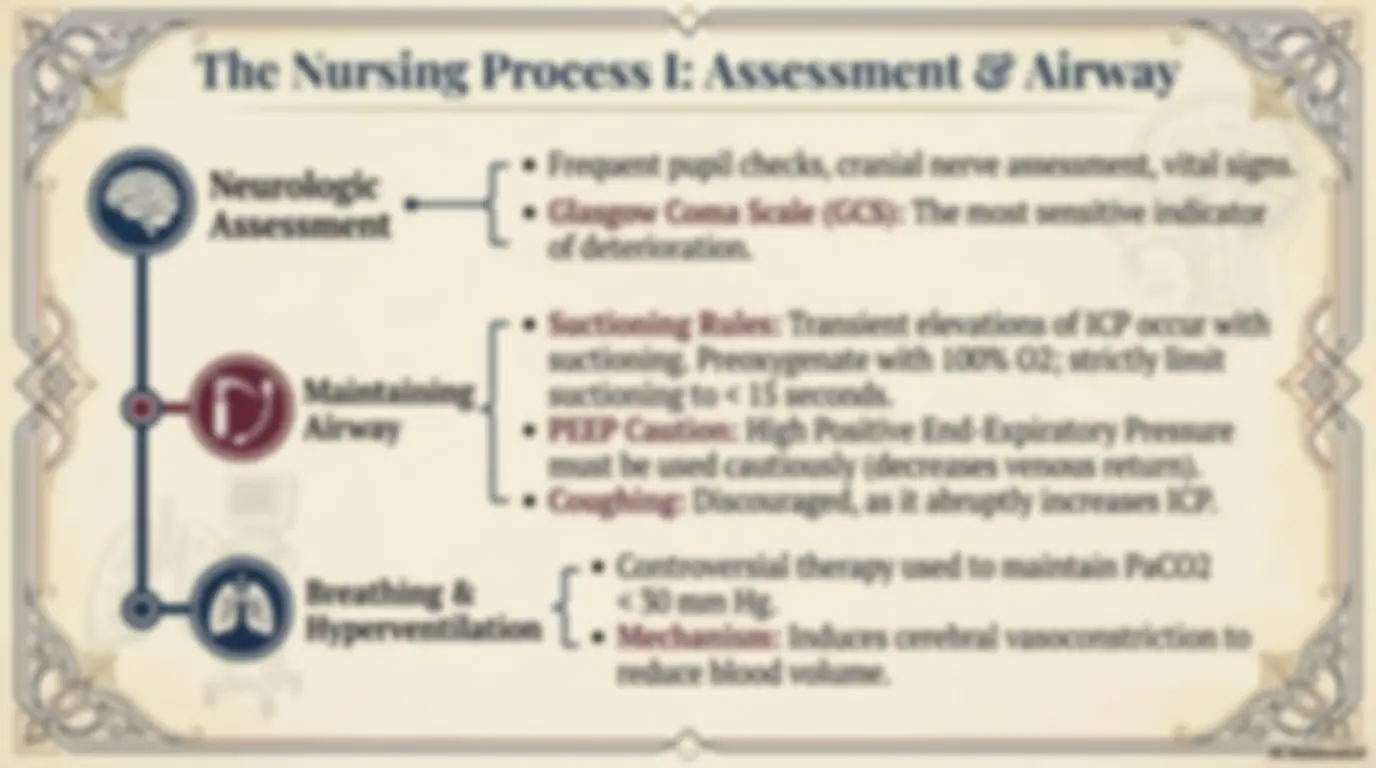
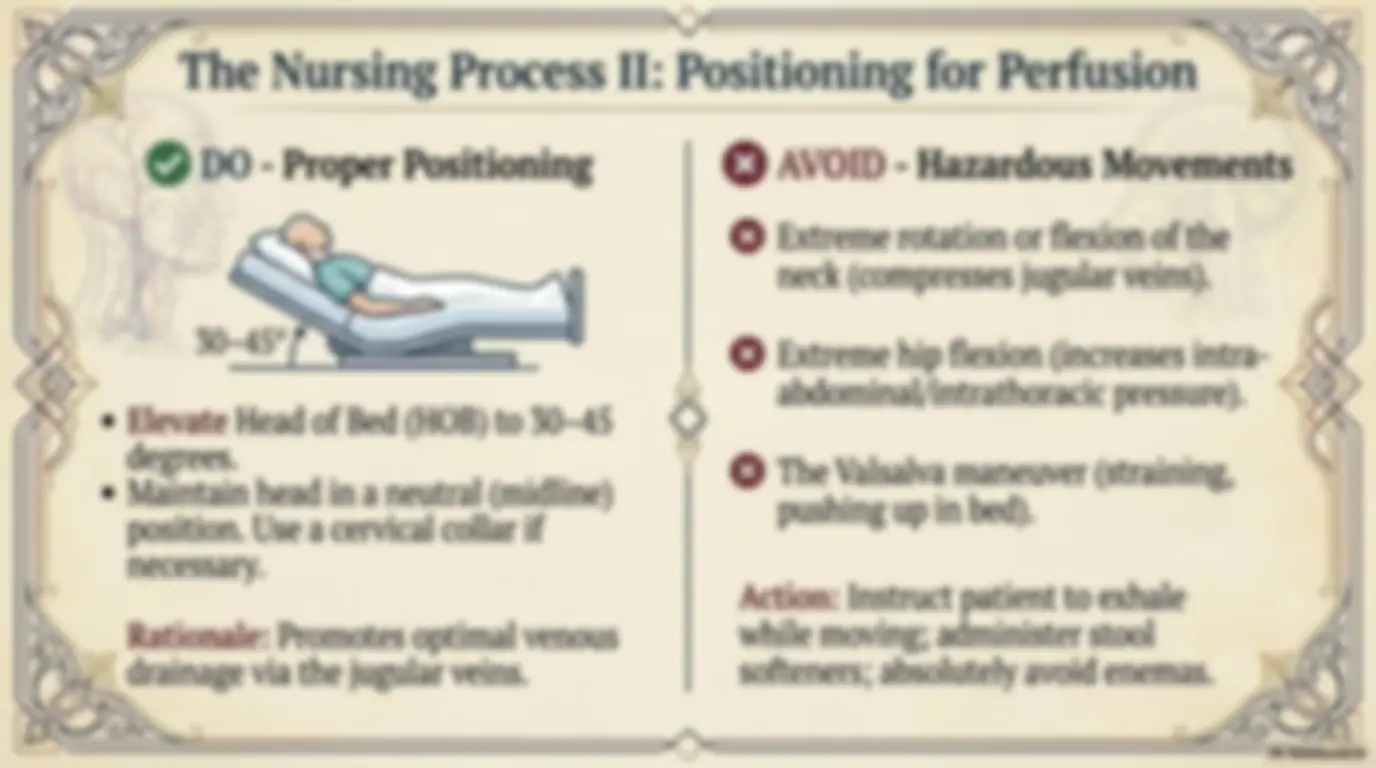
OP oe J » G S q o> KE XK XK omh}e DN an The Comprehensive Clinical Masterclass & Exam Guide ih Q Clinical © (| Manifestations Surgical Management Process WA) Brain Tissue (1400 g) Blood (75 mL) y; \ a Cerebrospinal J) — Fluid [csF} TF (75 mL) Z\ Normal Values Block ¢ Normal ICP: 0 to 10 mm Hg ¢ Upper limit of normal: 15 mm Hg Sy La ip we Nw The Monro-Kellie Doctrine Due to limited space in the rigid skull, an increase in one component requires a decrease in others to maintain equilibrium. Compensatory Mechanisms: ¢ Displacing/shifting CSF ¢ Increasing absorption or decreasing production of CSF « Decreasing cerebral blood volume Minor fluctuations occur normally via posture, ‘) coughing, or systemic 02/CO2 changes. Me HESS a 5 AAS a Pathophysiology: The Ischemic Cascade & Edema S 4) Step 1: Initial Insult Trauma, tumor, subarachnoid hemorrhage, or encephalopathy. if J i iL — Step 2: Cerebral Edema vy Abnormal fluid accumulation in intra/extracellular spaces. Brain tissue swells. _|| | l AY Fe Step 3: Decreased Perfusion Rising ICP reduces cerebral blood flow. Ischemia and cell death begin. f?} v7 Step 4: Loss of Autoregulation ., The brain loses its ability to adjust vessel diameter to maintain constant flow. aT — Step 5: Tissue Shift & Herniation A Extreme pressure causes brain tissue to shift to areas of lower pressure, cutting off blood supply entirely. N \\ cerebral blood A\\ flow (ischemia). e Mechanism: Vasomotor center triggers sympathetic response to increase arterial pressure and overcome ICP. e Signs: Increasing systolic BP, widening pulse pressure, reflex cardiac slowing. e Recoverable if treated rapidly. @r : _ Cushing’s Triad (Decompensation) | h | BRADYCARDIA: Ky] ' J HR<60 bpm SBP HYPERTENSION: “of t SBP > 160 mmHg A\ DBP —” Pulse Pressure Widening BRADYPNEA: RR<10bpm A (or irregular respirations) e Status: A grave sign indicating autoregulation failure and impending herniation. e The Triad: 1. Bradycardia 2. Hypertension (with widening pulse pressure) 3. Bradypnea (or irregular respirations) ; Assessment & Diagnostic Rules Primary Modalities (Do) ¢ CT Scanning and MRI (most common). ¢ Cerebral Angiography, PET, or SPECT. e Transcranial Doppler (assesses cerebral blood flow). ¢ Evoked Potential Monitoring (measures nerve tissue electrical potentials). ry 4 2 427" 42 FF 4 2. ar Ar Avoid Lumbar Puncture. ~\ Rationale: The sudden release of pressure in the lumbar area can create YS? a pressure gradient causing the brain to rapidly herniate downward. —76 RE a Intracranial Monitoring Hardware #f B. Subarachnoid screw A) Intraventricular sey (bolt) catheter | Be fe ~ | C. Intraparenchymal sensor 4. Fiberoptic Transducer 1. Ventriculostomy (Intraventricular Catheter) The gold standard. Inserted into lateral ventricle. Allows precise monitoring, CSF drainage, and instillation of meds. Risk: Infection, ventricular collapse. CE, 2. Subarachnoid Bolt (Screw) Hollow device through skull/dura. Avoids brain shift issues/small ventricles; no ventricular puncture. Risk: Blockage by clot. 3. Epidural Monitor Pneumatic flow sensor. Low infection rate; cannot withdraw CSF. 4. Fiberoptic Transducer Miniature transducer placed in subdural space/ventricle; reflects pressure as electrical signals. Gor A. oie &\ NotebookLM xx Medical Management I: Volume Reduction NG ») Osmotic Diuretics Corticosteroids q Intervention: Mannitol & Hypertonic Saline Intervention: Dexamethasone. (3%). Mechanism: Reduces edema surrounding Mechanism: Draws water across intact tumors. membranes to reduce brain volume. Nursing: Requires catheter; monitor serum (Note: Not used for head trauma). osmolality; watch for pulmonary edema. Fluid Restriction CSF Drainage Intervention: Maintain negative fluid balance. Intervention: Ventriculostomy drainage. Mechanism: Promotes dehydration and Mechanism: Removal of fluid restores CPP. hemoconcentration to pull fluid across osmotiqd Caution: Excessive drainage causes a ee Overhydration strictly avoided. ventricular collapse and herniation. & Le wN 2 <>< 2 A354 WZ SG xx Tees OI "4 Medical Management II: Perfusion, Demand & Siig Pillar 1: Optimizing Pillar 2: Reducing Pillar 3: Surgical Hemodynamics Metabolic Demand Intervention e Use fluid volume and ¢ Sedation/Barbiturate Coma: ¢ Decompressive inotropic agents High doses of pentobarbital or Hemicraniectomy: (dobutamine, propofol reduce brain oxygen Surgical removal of skull {U)) norepinephrine). demand. Requires intubation/ bone flap. ¢ Objective: Maintain continuous monitoring. ¢ Objective: Allows the adequate cardiac output. | ° Heras epg blank brain to expand without (© ¢ Target Metric: Keep Shien tony ides ankets. pressure constraints of CPP > 70 mm Hg. (increases 02 consumption). the cranial att K<(G\ Neurologic ! Assessment Maintaining Airway Breathing & Hyperventilation e Frequent pupil checks, cranial nerve assessment, vital signs. e Glasgow Coma Scale (GCS): The most sensitive indicator of deterioration. e Suctioning Rules: Transient elevations of ICP occur with suctioning. Preoxygenate with 100% O2; strictly limit suctioning to < 15 seconds. e PEEP Caution: High Positive End-Expiratory Pressure must be used cautiously (decreases venous return). e Coughing: Discouraged, as it abruptly increases ICP. e Controversial therapy used to maintain PaCO2 { < 30 mm Hg. ¢ Mechanism: Induces cerebral vasoconstriction to reduce blood volume. xx a Ze (The Nursing Process II: | © DO - Proper Positioning 30-45° e Elevate Head of Bed (HOB) to 30-45 degrees. e Maintain head in a neutral (midline) position. Use a cervical collar if necessary. N Rationale: Promotes optimal venous drainage via the jugular veins. NS Positioning for hatston Se €3 AVOID - Hazardous Movements €3 Extreme rotation or flexion of the neck (compresses jugular veins). © Extreme hip flexion (increases intra- abdominal/intrathoracic pressure). © The Valsalva maneuver (straining, pushing up in bed). Action: Instruct patient to exhale while moving; administer stool 6 AE Oo softeners; absolutely avoid enemas.