Partial preview of the text
Download Peritoneal dialysis PD and more Summaries Nursing in PDF only on Docsity!
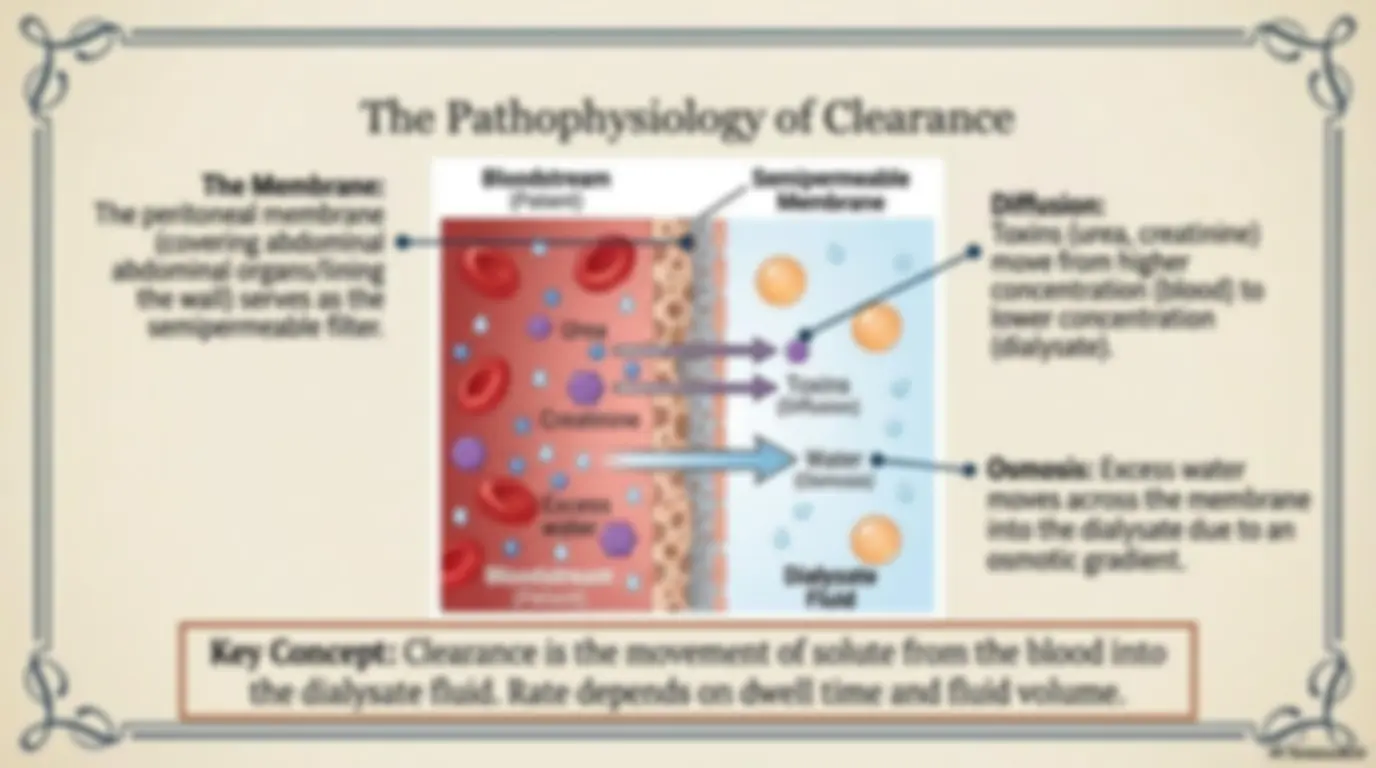
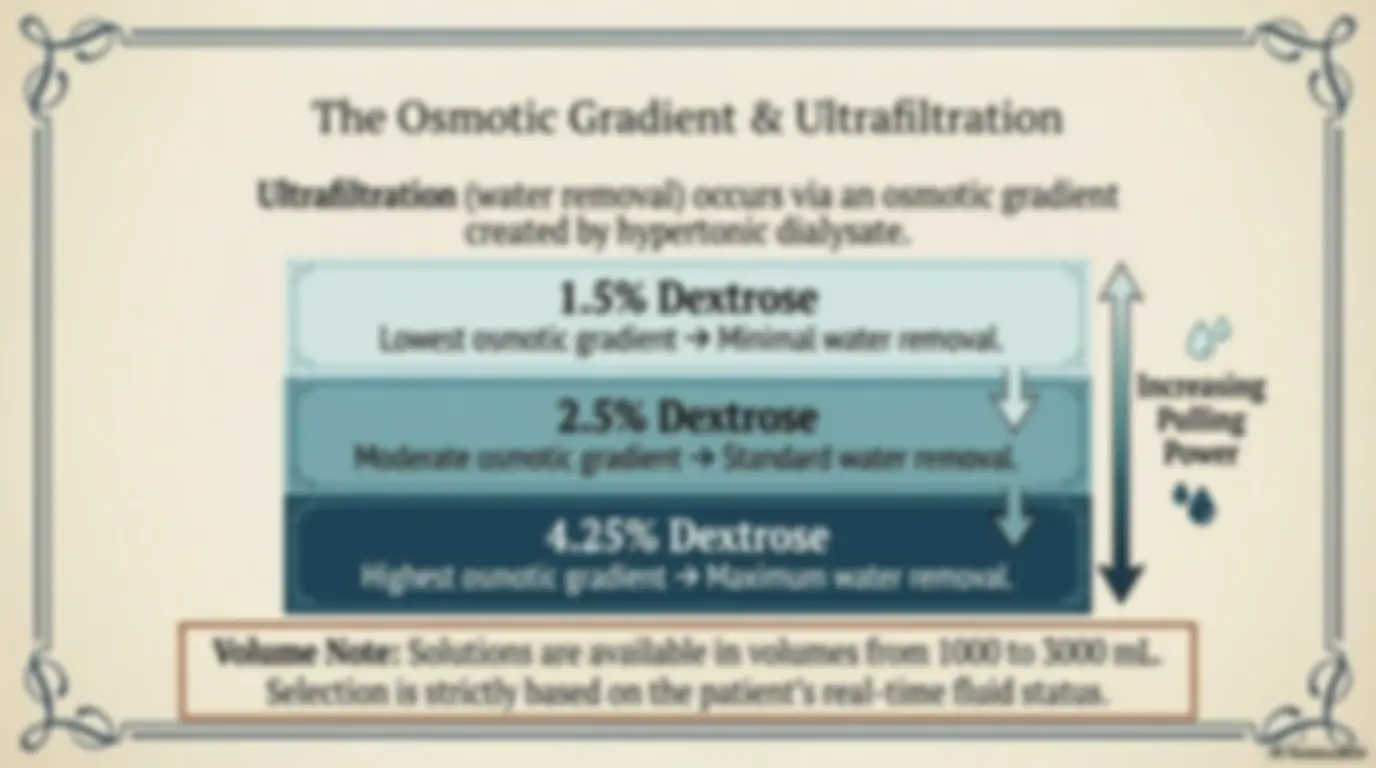
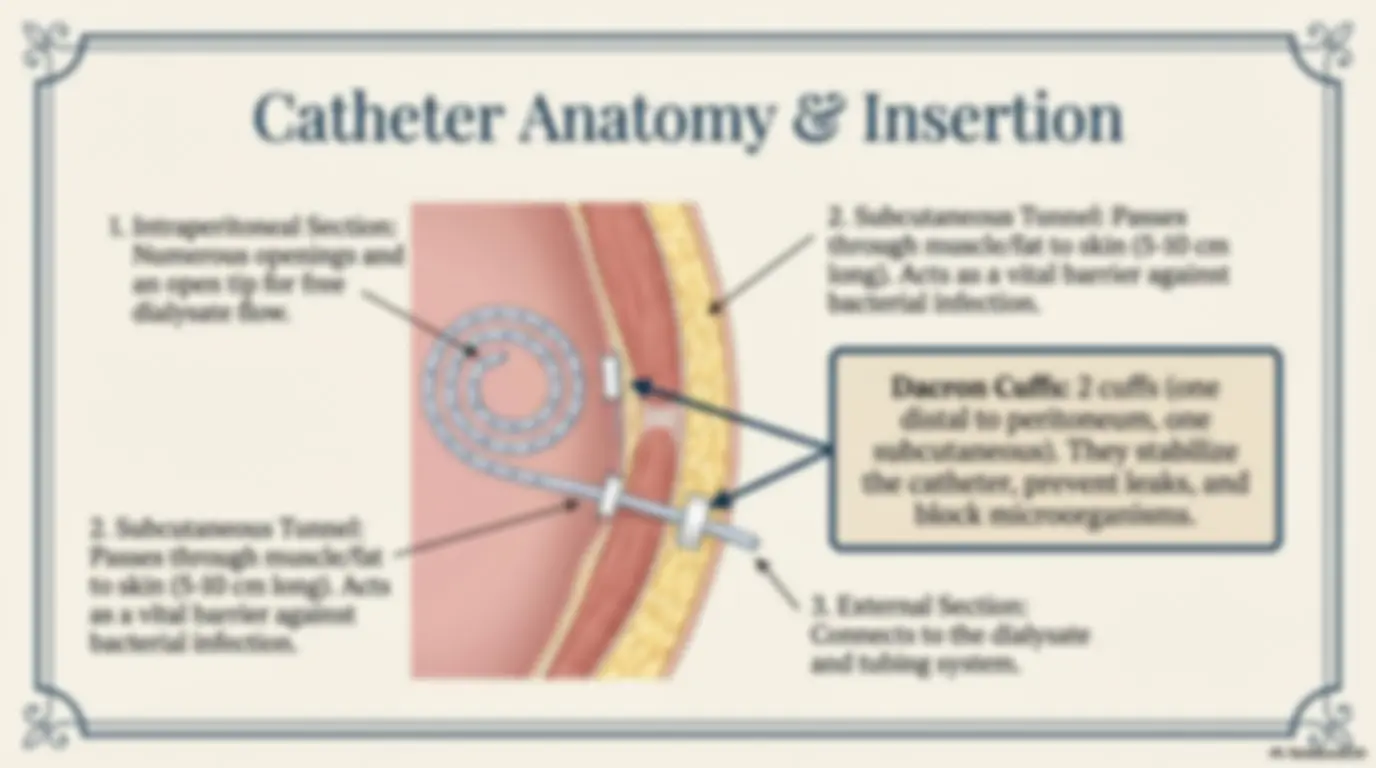
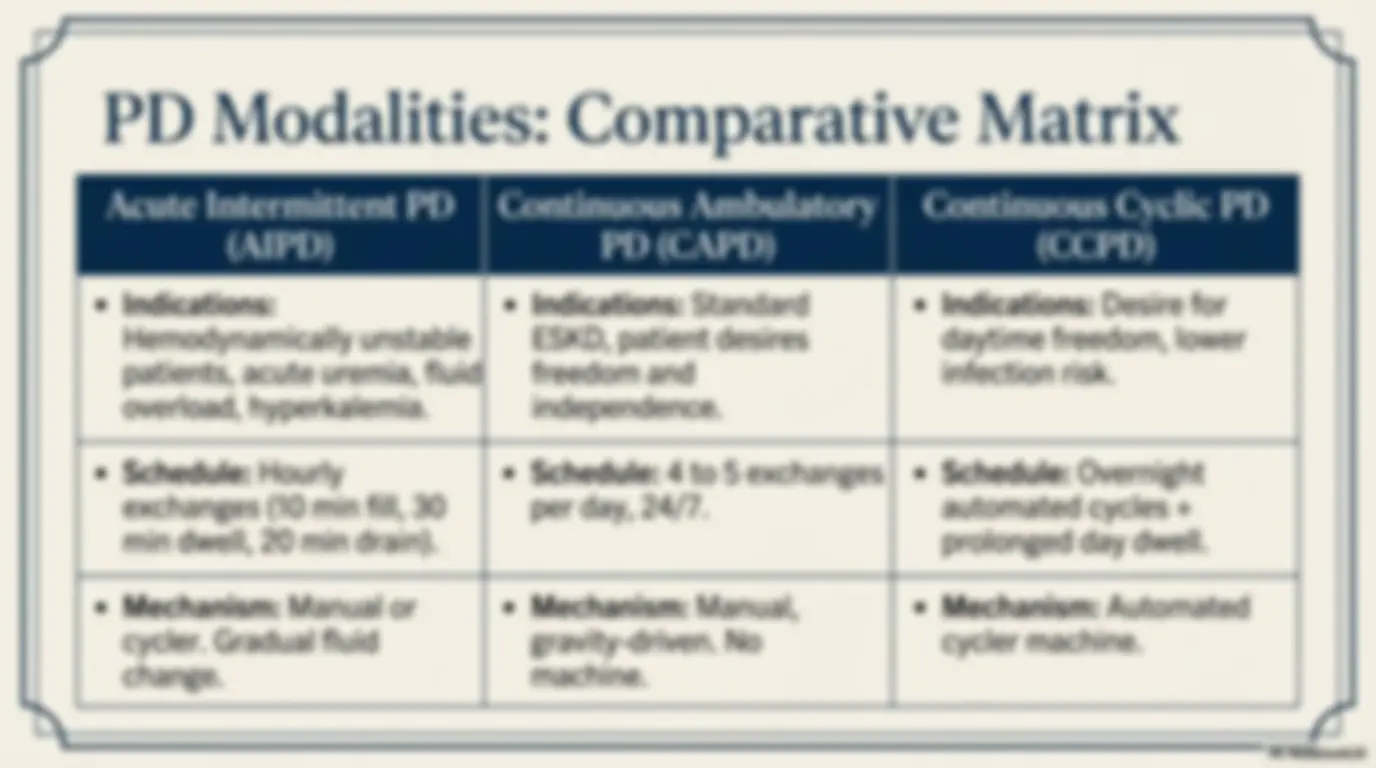
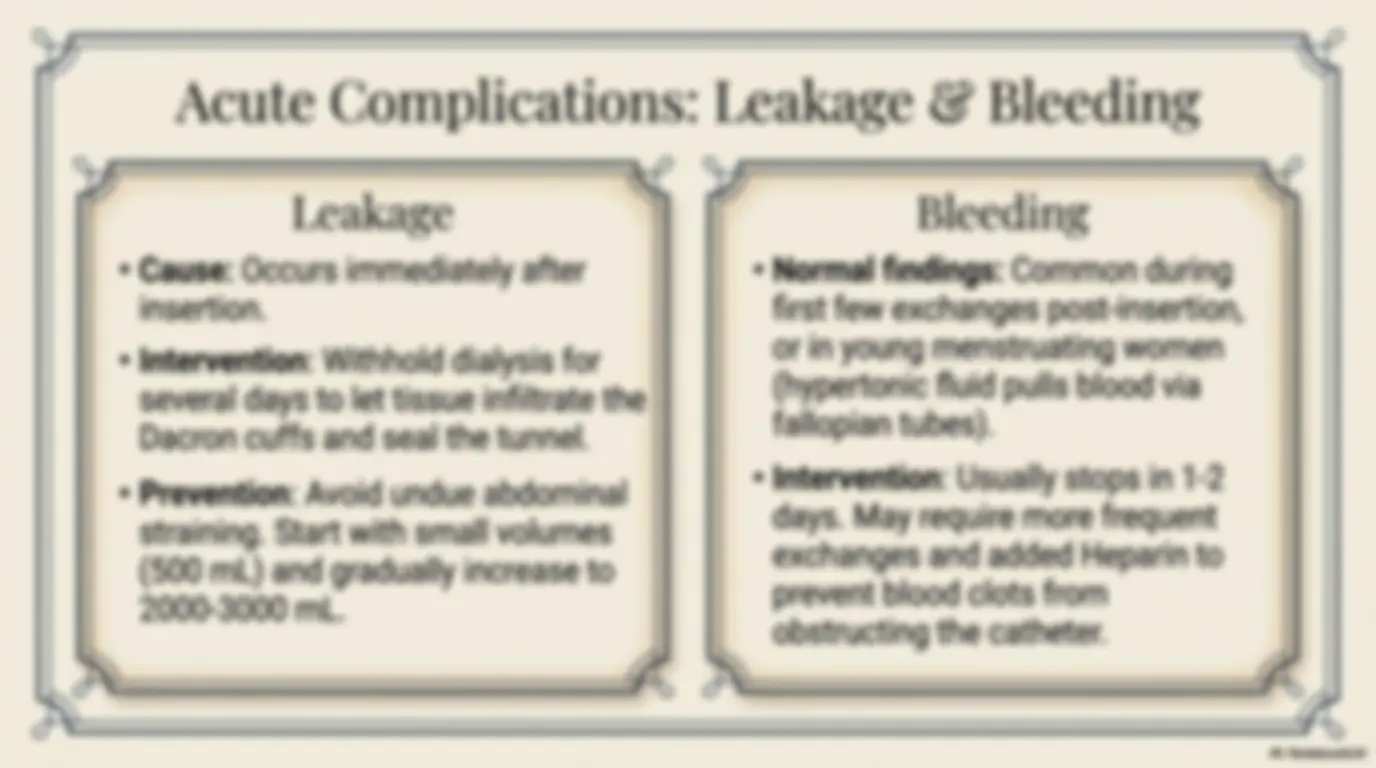
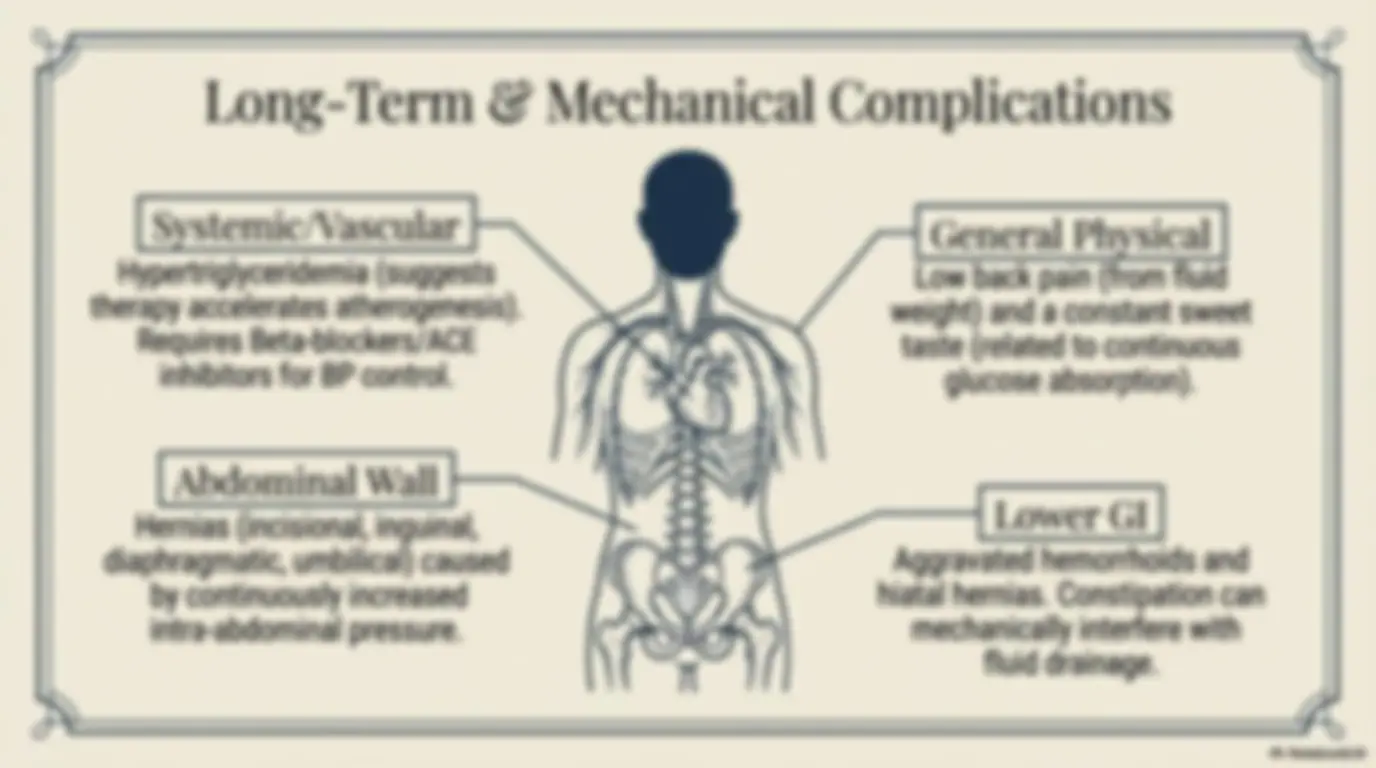
= Peritoneal Dialysis (PD) Renal Replacement Therapies | Exam Preparation Module | Urgent Dialysis Triggers Advanced CKD & ESKD Triggers | ¢ High/increasing serum potassium ¢ Uremic signs affecting all systems ¢ Fluid overload/impending (nausea, severe anorexia, pulmonary edema confusion) ¢ Increasing acidosis ¢ Fluid overload unresponsive to ¢ Advanced uremia diuretics ¢ Pericarditis (pericardial friction * Hyperkalemia rub) * General lack of well-being ¢ Medication toxicity/poisoning The Pathophysiology of Clearance \ The Membrane: Bloodstream Semipermeable The peritoneal membrane Liat j ion Membrane (covering abdominal abdominal organs/lining the wall) serves as the semipermeable filter. Diffusion: Toxins (urea, creatinine) do @ move from higher ! @ concentration (blood) to () lower concentration (dialysate). ° — a al Toxins Gg (Diffusion) OI ! sill y >a Osmosis: Excess water moves across the membrane ia into the dialysate due to an osmotic gradient. Bloodstream , o *65( Dialysate (Patient) —— BAA olay Fluid Key Concept: Clearance is the movement of solute from the blood into We the dialysate fluid. Rate depends on dwell time and fluid volume. The Osmotic Gradient & Ultrafiltration | Ultrafiltration (water removal) occurs via an osmotic gradient | created by hypertonic dialysate. 1.5% Dextrose c Lowest osmotic gradient > Minimal water removal. (° | Ese |] Increasing 2.5% Dextrose Vv _ |) Pating Moderate osmotic gradient > Standard water removal. Power ak ) 4.25% Dextrose . Highest osmotic gradient > Maximum water removal. | Volume Note: Solutions are available in volumes from 1000 to 3000 mL. Selection is strictly based on the patient’s real-time fluid status. Clinical Preparation Protocol f Patient Prep Fluid Prep (Warming Rules) 1. Empty bladder and bowel {jz ° Why Warm?: Prevents abdominal (reduces risk of internal organ © pain/cramping, dilates peritoneal puncture during insertion). vessels to increase urea clearance. $5 _» APPROVED: Dry heating (heating 2. Administer broad-spectrum cabinet, incubator, heating pad). antibiotics to prevent infection. » DANGER / DO NOT USE: Microwave oven (danger of burning peritoneum) or warm water baths (introduces bacteria to bag exterior, causing peritonitis). ia 3. Catheter typically placed on nondominant side for easier self-care access. Microwave oven (danger of burning peritoneum) or warm water baths (introduces bacteria to bag exterior, causing peritonitis). &A\ NotebookLM 1, Intraperitoneal Section: Numerous openings and an open tip for free dialysate flow. 2. Subcutaneous Tunnel: Passes through muscle/fat to skin (5-10 cm long). Acts as a vital barrier against bacterial infection. 2. Subcutaneous Tunnel: Passes through muscle/fat to skin (5-10 cm long). Acts as a vital barrier against bacterial infection. Dacron Cuffs: 2 cuffs (one distal to peritoneum, one subcutaneous). They stabilize the catheter, prevent leaks, and block microorganisms. AN 3. External Section: Connects to the dialysate and tubing system. PD Modalities: Comparative Matrix Acute Intermittent PD | Continuous Ambulatory e Indications: Hemodynamically unstable patients, acute uremia, fluid overload, hyperkalemia. PD (CAPD) e Indications: Standard ESKD, patient desires freedom and independence. Continuous Cyclic PD (CCPD) e Indications: Desire for daytime freedom, lower infection risk. e Schedule: Hourly exchanges (10 min fill, 30 min dwell, 20 min drain). e Schedule: 4 to 5 exchanges | per day, 24/7. e Schedule: Overnight automated cycles + prolonged day dwell. e Mechanism: Manual or cycler. Gradual fluid change. e Mechanism: Manual, gravity-driven. No machine. e Mechanism: Automated cycler machine. A\ NotebookLM Executing CAPD: The “Y-Shaped” System Continuous progress -> Less extreme laboratory value fluctuations than HD. Fresh peritoneal dialysate . Based on provided reference Effluent collection bag aye Setup: Branch 1 = Full dialysate bag. Branch 2 = Sterile empty bag. Branch 3 = Transfer set on patient catheter. $9 Asepsis: G Hand hygiene, don mask. Connect open end of “Y” to transfer set. Ly Infuse: Instill dialysate -> Clamp transfer set -> Make it a closed system. Drain: Unclamp later to drain effluent into the empty bag over 20-30 mins. xp Safety Note: Whenever a connection/disconnection is made, anyone within 6 ft must wear a mask to prevent airborne bacteria contamination. us A\ NotebookLM Leakage ¢ Cause: Occurs immediately after insertion. ¢ Intervention: Withhold dialysis for several days to let tissue infiltrate the Dacron cuffs and seal the tunnel. ¢ Prevention: Avoid undue abdominal straining. Start with small volumes (500 mL) and gradually increase to 2000-3000 mL. ; Bleeding ¢ Normal findings: Common during first few exchanges post-insertion, or in young menstruating women (hypertonic fluid pulls blood via fallopian tubes). ¢ Intervention: Usually stops in 1-2 days. May require more frequent exchanges and added Heparin to prevent blood clots from obstructing the catheter. Al NotebookLM Systemic/Vascular Hypertriglyceridemia (suggests therapy accelerates atherogenesis). Requires Beta-blockers/ACE inhibitors for BP control. Abdominal Wall Hernias (incisional, inguinal, diaphragmatic, umbilical) caused by continuously increased intra-abdominal pressure. Ww N D | L ong-Term & Mechanical Complications General Physical Low back pain (from fluid weight) and a constant sweet taste (related to continuous glucose absorption). Aggravated hemorrhoids and hiatal hernias. Constipation can mechanically interfere with fluid drainage. 3 | AN A\ NotebookLM the first month from dialysate glucose). \ Fluids & Potassium (Unrestricted) Normal fluid intake is permitted because patients continuously lose 2-3 L of fluid per 24 hours. Pt/sodium restrictions are rarely needed (unlike hemodialysis). Carbohydrates (Regulated) Limit carbs to avoid excessive weight gain (patients commonly gain 3-5 Ibs in High-protein diet required to compensate for massive protein losses through the peritoneal membrane during Increased daily fiber intake is mandatory to prevent constipation (which impedes dialysate flow). Protein (High) continuous dialysis. Fiber (High) 0 A\ NotebookLM Psychosocial Needs & Body Image - Altered Body Image Presence of abdominal catheter, bags, and cycler. Waist size +> increases by 1-2 inches with fluid, altering clothing fit and = Causing patients to feel “fat”. ~ Sexuality & Intimacy Catheter feels physically and psychologically “in the way”. | ° A full abdomen (2L fluid) and the t f bedside cycler can interfere with \ sexual function and intimacy. ‘Burnout & Depression Patients may feel crushed a by the continuous, 24/7 mi. responsibility of self-care S and lack offreetime. 7 Interventions ) Facilitate peer support (talking e eto successfully adapted patients). Do not label patients as “noncompliant” without assessing coping strategies. ye 0 A\ NotebookLM Hospitalized Care: Protecting Vascular Access Key Concept: Access failure is the #1 cause of hospital admissions for chronic dialysis patients. Strict Restrictions for the Access Arm - NO blood pressure measurements. - NO blood draws or IV insertions. ( - NO tight dressings, restraints, or jewelry. Assessment Protocol & Usage s - Evaluate for the presence of a palpable “thrill” or audible “bruit” every shift. Absence indicates blockage/clotting. - Device is exclusively for dialysis. Only a dialysis nurse or physician may cannulate in emergencies. Ay NotebookLM Hospitalized Care: Critical Acute Monitoring Warning 1: Intravenous Therapy Danger Rule: IV fluid administration rate must be as slow as possible. Pathology: Because anuric patients cannot excrete water, rapid IV fluids instantly result in pulmonary edema. Evaluate all lV meds for hidden potassium/magnesium. Warning 2: Uremic Pericarditis & Tamponade Detection: Assess for substernal chest pain, low-grade fever, and a pericardial friction rub. Pulsus Paradoxus: Look for a drop in BP >10 mmHg during inspiration. Progression: If progressing to life-threatening cardiac tamponade, watch for narrowing pulse pressure, muffled heart sounds, and hypotension. Ensure BP meds are withheld before any acute dialysis sessions. Ay NotebookLM