Download Respiratory Physiology: Structure, Function, and Lung Volumes and more Study notes Physiology in PDF only on Docsity!
STRUCTURE AND FUNCTION
prime function is exchange of O 2 and CO 2 other functions, a. blood reservoir b. heat exchange c. metabolism - synthesis & catabolism d. immunological and mechanical defence
blood/gas barrier to diffusion ~ 50-80 m^2 alveolar walls have two sides, a. active side → ∼ 0.4 μm b. service side → ∼ 1-2 μm
(Nunn) ~ 200-600 million alveoli, depending upon height and size each alveolus ~ 0.2 mm in diameter at FRC, and is actually polyhedral not spherical blood/gas interface established by ventilation of airways and perfusion
Cell Types in the Respiratory Tract
a. Capillary endothelium - form calveoli ~ 0.1 um thick by 126 m^2 b. Alveolar type I cells - also 0.1 μm thick
- have 1 nm gap junctions
- impermeable to albumin
- allow extravasation of mφ's
- unable to divide
- highly sensitive to hyperoxia c. Alveolar type II cells - rounded cells at septal junctions
- produce surfactant
- resistant to hyperoxia d. Alveolar type III cells? function = "brush" cells e. Alveolar macrophages - (mφ) present in alveoli & airways
- normal defence & scavenging f. PMN's - not usually present
- seen in smokers & 2° to NCF g. Mast Cells h. Non-ciliated bronchial epithelial, "Clara", cells i. APUD cells
AIRWAYS AND FLOW
Main Airway Branches & Zones
trachea R+L main bronchi
conducting zone generations 1-
lobar bronchi segmental bronchi bronchioles terminal bronchioles
respiratory bronchioles respiratory zone
- primary lobule / or acinus generations 17-
alveolar ducts atria alveolar sacs
CZ doesn't contribute to gas exchange → anatomical dead space RZ (including transitional zone) → most of lung volume ~ 3000 ml air flow → terminal bronchioles by (^) bulk flow then due to large increase in X-sectional area, flow v decreases and movement is by diffusion within an acinus distances are short, ≤5 mm, and diffusion is rapid, ≤1 sec alveolar stability is maintained by surfactant air velocity decreases at terminal bronchioles , these are often a site of collection of foreign matter a normal tidal breath of ~ 500 ml requires δP ~ 3 cmH 2 O due to high the compliance of lung tissue and low resistance to gas flow,
gas flow 1.0 l/s → δP ~ 2 cmH 2 O
this equates to a compliance, C ~ 180 ml/cmH 2 O
BLOOD VESSELS AND FLOW
initially arteries, veins and bronchi run together toward the periphery, veins → outside of primary lobules bronchi & arteries → center
capillaries ~ 7 μm diameter and are short → large surface area (SA) the pulmonary bed receives the entire CO, excluding true shunt flow the mean pulmonary arterial pressure ~ 15 mmHg RBC's traverse the capillary bed in ~ 0.75 sec and traverse ~ 3 alveoli the bronchial circulation supplies down to the terminal bronchioles but only a small fraction of this blood supply drains → pulmonary veins
Measurement of FRC and RV
NB: these volumes cannot be measured by spirometry , as they contain gas which cannot be expelled from the lungs
Functional Residual Capacity
Def'n: the volume of gas left in the lungs at the end of normal tidal expiration
FRC is the lung volume in which gas exchange is taking place small fluctuations of alveolar and arterial gas tensions occur with each tidal breath as fresh gas mixes with alveolar air
FRC therefore acts as a buffer ,
- maintaining relatively constant A & a gas tensions with each breath
- preventing rapid changes in alveolar gas with changes in ventilation or inspired gas, eg. during induction or recovery from anaesthesia
- increasing the average lung volume during quiet breathing, reducing work of breathing due to shape of compliance curve
methods of measurement,
- closed circuit helium dilution
- closed circuit nitrogen washout
- body plethysmograph
Closed Circuit Helium Dilution
rebreathing takes place from a spirometer of known volume (V 1 ) and helium concentration (C 1 ) as He is relatively insoluble in blood, it therefore equilibrates between the lung and spirometer volumes are calculated by conservation of mass , ie. C 1 × V 1 = C 2 × (V 1 +V 2 ), depending upon the starting point,
i. from end tidal expiration → FRC ii. from end forced expiration → RV
NB: in some types of pulmonary disease areas of lung are poorly, or unventilated, therefore will result in underestimation ie. only communicating volume is measured
Closed Circuit Nitrogen Dilution
using N 2 washout, the patient breaths 100% O 2 if the alveolar N 2 = 80% and the volume of N 2 collected is 4.0 l, then the initial lung volume must have been 5.0 l relies upon N 2 being relatively insoluble and moving slowly from blood to alveolar air
Body Plethysmograph
includes both communicating and non-communicating thoracic gas volume the later includes both non-ventilated lung and extrapulmonary gas the subject, in an air-tight box, breathes through a mouthpiece which closes at end expiration and the subject inhales against closed airway
Using Boyle's Law : PV = K at constant T
Pb1.Vb1 = Pb2.(Vb1 - δV), where δV applies for the box & lung
PL1.VL1 = PL2.(VL1 + δV), where VL1 = FRC
thus,
FRC =
PL 2 ×δ V PL 1 −^ PL 2
Factors Affecting FRC
- body size - FRC ∝ height (~ 32-51 ml/inch)
- sex - females ~ 90% of male FRC (= height)
- age - work by Nunn → no correlation!
- others have shown small increase
- diaphragmatic muscle tone originally, FRC believed to = equilibrium for lung/chest wall system diaphragmatic tone maintains FRC ~ 400 ml above true relaxed state → ↓ FRC with anaesthesia
- posture - ↓ FRC in the supine position ~ 0.5-1.0 l
- lung disease i. loss of lung ER with emphysema → ↑ FRC ii. increased expiratory resistance with asthma & external apparatus → ↑ FRC
- chest wall - increased abdominal contents → ↓ FRC
- alveolar-ambient pressure gradient * PEEP increases the FRC
Residual Volume
Def'n: the volume of gas in the lung at the end of maximal expiration
determined by the balance of expiratory muscle activity and the resistance to volume decrease by the lungs and chest wall
Vital Capacity
Def'n: the maximum volume that can be exhaled following a maximal inspiration
VC = IRV + TV + ERV VC and its components are measured by spirometry , either bell (Benedict-Roth), or wedge variations in VC occur with,
- height, weight and surface area - VC roughly proportional to height
- age - ↓ VC with increasing age
- sex - M > F
- posture - less when supine, cf. sitting or standing
Reductions of Vital Capacity
- Pulmonary reductions in the distensibility of lung tissue reductions in the absolute volume of lung, (obstruction, atelectasis, pneumonia)
- Non-pulmonary these may be due to limitation of, i. respiratory movements - neuromuscular ii. thoracic expansion - musculoskeletal, position iii. diaphragmatic descent - pregnancy, obesity, ascites, etc. iv. expansion of lung - occupying intrathoracic space
a reduction in VC occurs in many diseases, however by itself doesn't signify pulmonary disease, eg. VC may be normal in emphysema normal values,
- IC ~ 75% of VC ( = TV + IRV)
- ERV ~ 25% of VC
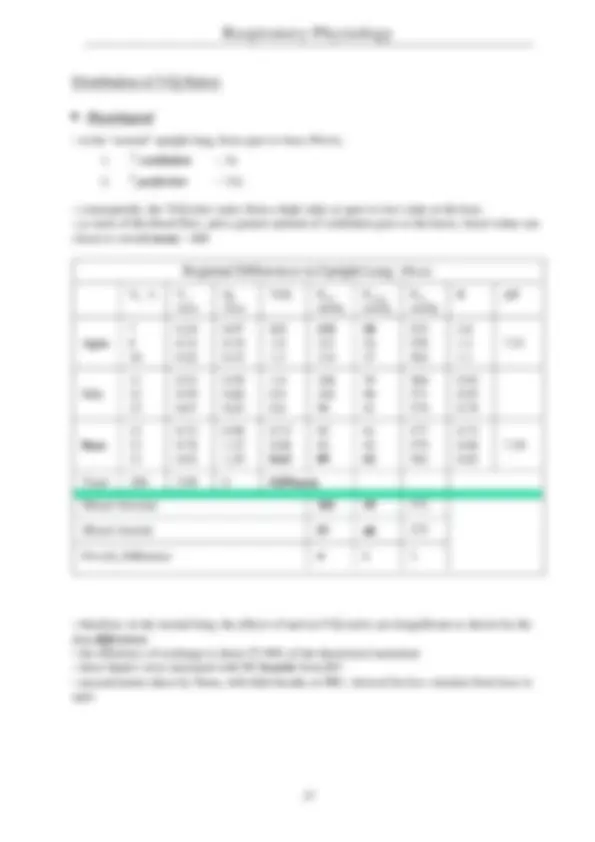
Alveolar Gas Tensions
i. PaO2 ~ 101 mmHg ii. PaCO2 ~ 40 mmHg
assuming PICO2 = 0, and since there is no gas exchange in VDPhys^ , then
VCO2 = VA × FACO2 , where FACO2 = %CO 2 / 100 ml
at end-tidal gas approximates alveolar gas, then,
VA = VCO2 / FE'CO2 , gaining FE'CO2 from an IR analyser
as PCO2 is directly proportional to FCO2 , so
NB: in normal subjects alveolar and arterial PCO2 are virtually equal
Anatomical Dead Space VDAnat
Def'n: the volume of the^ conducting airways in which no gas exchange takes place, or
that part of the inspired volume which is expired unchanged at the beginning of expiration, or
"the volume of gas exhaled before CO 2 reaches the alveolar plateau - according to Fowler (1948)" (Nunn - now the commonly used definition)
also termed the series dead space and is equal to the boundary between convective gas transport and diffusion
the two commonly used methods of measurement are,
- Fowler's method - tracer washout
- Bohr's method - conservation of mass
PaCO 2 ∝
V
CO 2 VA
Fowler's Method
single breath analysis using an indicator gas ( N 2 ,CO 2 , O 2 , He) to mark the transition between dead space and alveolar gas following inspiration of 100% O 2 , a plot of VEXP vs. %[N 2 ] → wash-in phase the mid-point of the wash-in (where area A = area B below) measures the transition from conducting airways to the transition from dead space to alveolar gas in patients with non-uniform distribution of ventilation, ie. regions of the lung with different time constants , a slow "wash-in" is seen and the method is inaccurate
Factors Affecting Anatomical Dead Space
- Body Size - ↑ VDAnat^ with increasing body size
- in ml ~ lean body weight in lb, or ~ 2.2 ml/kg
- Age - ↑ VDAnat^ with increasing age (?VD/VT)
- Lung Volume - ↑ VDAnat^ with increasing volume ~ 20 ml/l increase in lung volume from FRC
- Posture - ↓ VDAnat^ with supine posture → supine ~ 101 ml sitting ~ 147 ml (Fowler)
- Respiratory Flow Pattern decreased, using Fowler technique, with low VT due to the mixing affect of the heart beat below the carina, and the cone advance of laminar flow, seen at low flow velocities
- Hypoxia §^ - bronchoconstriction → ↓ VDAnat
- Drugs and Anaesthetic Gases §^ - bronchodilatation → ↑ VDAnat
- Lung Disease - emphysema → ↑ VDAnat
- loss or excision of lung → ↓ VDAnat
- Endotracheal Intubation - ↓ VDAnat^ ~ 50%
- but there is the additional volume of the circuit
- Position of the Jaw & Neck - increases with jaw protrusion in non-intubated subjects
NB: §minimal effects
Alveolar Dead Space VDAlv
Def'n: that part of the inspired gas which passes through the anatomical dead space and enters alveoli, however is ineffective in arterialising mixed venous blood
also termed parallel dead space
does not represent the actual volume of these alveoli the cause is failure of adequate perfusion of the alveoli to which gas is distributed, a. alveoli with no perfusion → V/Q infinite b. alveoli with reduced perfusion → V/Q > 0.
the separation of alveoli into these two groups = Riley analysis normally is minimal in healthy subjects but increases with disease
Factors Affecting Alveolar Dead Space
- Age - ↑ VDAlv^ with increasing age
- Pulmonary Arterial Pressure a decrease in PA pressure (eg. hypotension) decreases perfusion to the upper parts of the lung → ↑ zone 1 & ↑ VDAlv
- Posture VDAlv^ increases in the upright and lateral positions due to exaggeration of hydrostatic differences → ↑ zone 1 this is theoretical, no data is available (Nunn)
- IPPV increases VDAlv^ due to exaggeration of hydrostatic failure of perfusion also decreases total pulmonary blood flow applied wave-form IPPV with short inspiration (t < 0.5 s), → increases VDAlv^ due to maldistribution of ventilation
- Tidal Volume - as VT increases, so VDAlv^ increases but the ratio remains constant
- Oxygen - hyperoxic vasodilatation → ↑ VDAlv
- hypoxic vasoconstriction → ↓ VDAlv
- Anaesthetic Gases - ↑ VDAlv^ but not known why!
- Lung Disease - ↑ VDAlv^ increased in multitude of diseases i. ARDS → microemboli & ventilation of non-vascular air spaces ii. IPPV & lateral posture → gross V/Q mismatch
Physiological Dead Space
Def'n: VDPhys^ = Total Dead Space = VDAlv^ + VDAnat
or, that part of the tidal volume which does not participate in gas exchange and is ineffective in arterialising mixed venous blood, because either,
- it doesn't reach the alveoli - VDAnat
- it reaches alveoli with no capillary flow, or
- it reaches alveoli with inadequate flow - VDAlv
in normal supine man, VDAlv^ ~ 0, therefore,
VDPhys^ ~ VDAnat^ ~ 150 ml
Measurement of Physiological Dead Space
using the Bohr Equation to measure VD, the value for alveolar CO 2 is taken as the ETCO 2 if "ideal" alveolar PCO2 is taken as arterial PaCO2, then the equation yields physiological dead space,
VDAnat/VT = (FACO2 - FECO2 ) / FACO2 the Bohr Equation
but since PX and FX are proportional, then
VD/VT = (PACO2 - PECO2 ) / PACO2 where PA is end-expired
substituting PaCO2 as the ideal alveolar value,
Enghoff Modification (1938)
*** normally = 0.2 to 0.**
this ratio is more useful as it tends to remain constant, c.f. the actual value for VDPhys^ which may vary widely with changing tidal volumes expired gas is collected in a Douglas bag and the difficulty is getting only expired gas due to difficulties in the measurement of this, clinically the relationship between PaCO2 and ventilation is used, ie.
PaCO2 ∝ VCO2 / VA
VD
Phys
VT
=
PaCO 2 − PECO
2
PaCO 2
DIFFUSION
Def'n: the constant random thermal motion of molecules, in gaseous or liquid phases, which leads to the net transfer molecules from a region of higher concentration to a region of lower concentration (thermodynamic activity)
Fick's Law
Def'n: the rate of transfer of a gas through a sheet of tissue is,
a. proportional to the area available for transfer b. proportional to the gas tension difference c. inversely proportional to the tissue thickness
NB: where D = the diffusion constant
Determinants of Gas Diffusion
- Characteristics of the Gas
- Pressure Gradient
- Membrane Characteristics
Characteristics of the Gas
a. Molecular Weight V ∝ 1/√MW
Graham's Law : relative rates of diffusion are inversely proportional to the square root of the gas molecular weight
thus, lighter gases diffuse faster in gaseous media than heavier gases lighter molecules for given energy have faster velocities therefore, O 2 diffuses more rapidly than CO 2 in the gas phase (1.17 : 1) in health, diffusion distances in the alveoli are small (< 100 μm), however where distances are increased, regional differences in PO2 can occur this is only of importance in the gaseous pathway from ambient air to blood
V
. gas =^
A. D
T
×( Pgas 1 − Pgas 2 )
with either a lower PaO2 , or an impairment of diffusion (alveolar-capillary block) equilibrium may not be reached this will be exacerbated by conditions of increased CO, where the transit time is reduced the diffusion path is composed of a number of segments, a. at FRC, alveolar diameter ~ 200 μm → diffusion ~ 10 ms b. alveolar + capillary membrane on "active side" ~ 0.5 μm c. pulmonary capillaries ~ 7 μm (~ rbc) d. oxygenation of Hb
therefore, the diffusion path within the RBC is greater than across the lung the oxygenation of Hb is sufficiently slow to be the rate limiting step
Diffusing Capacity (DC)
Def'n: the rate of gas transfer / partial pressure difference for the gas
→ δQ / δPGAS
the term is comparable with electrical conductance for oxygen this becomes,
DCO2 = MRO 2 / (PcO2 - PaO2)
as it is impossible to measure the mean PcO2, an approximation is the Bohr integration procedure, by assuming,
a. the end PcO2 - PaO2 difference b. the rate of transfer of gas ∝ δPO 2 along the capillary → mean value by integration
however, this has been shown to be false, as assumption (b) doesn't hold true ie. the rate of uptake of O 2 by Hb is a non-linear function of the δPO 2 , depending upon the state of oxygenation of Hb factors which will reduce the diffusing capacity are, a. decreased capillary transit time ∝ ↑ CO b. decreased capillary blood volume c. pulmonary congestion d. alveolar capillary block
NB: V/Q mismatch is indistinguishable from decreased diffusing capacity
Diffusing Capacity for Carbon Monoxide
this is used as a substitute for oxygen, due to the intractable difficulties in measuring DCO it is convenient as the diffusion barrier is the same but the affinity of Hb for CO is so high that the mean PcCO can be ignored, and the equation simplifies to,
DCCO = CO uptake / alveolar PCO
the differences in the solubility and vapour densities of the two gases are such that the diffusion rate, to the point of entry into the RBC, for O 2 is ~ 1.23 times that of CO although the affinity of CO for Hb is ~ 250 times that of O 2 , the reaction rate is in fact slower, and is affected by the FIO 2 thus, by altering the FIO 2 , the different components of diffusion resistance to CO can be studied (solving simultaneous equations for below)
the second component, within the RBC, is not really a matter of diffusion but a product of the pulmonary capillary blood volume (Vc) and the reaction rate with Hb (rate = θ) thus, the total diffusing capacity, analogous to conductance , is given by,
1/DCL = 1/DCM + 1/(Vc.θ)
and, under similar conditions → (^) DCMO2 ~ 1.2 × DCMCO
methods for the measurement of DCCO include,
- steady state subject breaths 0.3% CO for 1 minute alveolar PCO is calculated from modified alveolar air equation uptake is from inspired & expired FCO by IR analysis
- (^) single breath VC breath of (0.3% CO + 10% He) held for 10 s no He enters blood, thus ratio FI/FE gives concentration of CO and the alveolar PCO from the FECO
- rebreathing same mixture as (b) rebreathed from reservoir