Comprehensive Study Guide D345
1
Summary WGU D345 Comprehensive Study Guide:
Dr Cole Remediation for OA
2026 update
Section 1 Highlight Guide
•
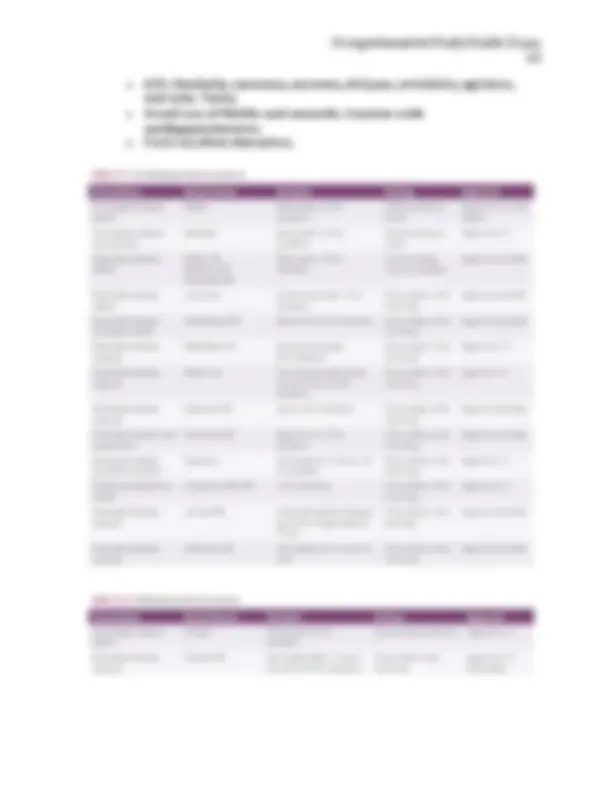
1. Neurotransmitters: know all the neurotransmitters, the role of
various neurotransmitters in various diagnosis and symptoms.
Recommendation: Make a chart with various diagnosis and the role
various neurotransmitters play in that diagnosis/symptom.
•
The study of the magnitude and variation of drug response is the
definition of
pharmacodynamics
.
Psychodynamics
is the study of
what the body does to a drug and helps explain the relationship
between the dose and response.
o
Dopamine produced in substantia nigra and ventral tegmental
area
▪
D: Drive/Drugs
▪
O: psychOsis
▪
P: Prolactin Inhibition
▪
A: Attention
▪
M: Motivation
▪
I: Involuntary Movements
▪
N: Nausea
▪
E: Energy
o
Serotonin is produced mostly in Raphe nucleus
▪
DOMAINS: Depression, Obsession, Migraines, Anxiety,
Intestines, Nausea, and Sexual.
▪
Serotonin Syndrome:
Shits and SHIVERS.
Shits(diarrhea), Shivering, Hyperreflexia, Increased
temperature, Vital sign instability, Encephalopathy,
Restlessness, and Sweating.
o
Norepinephrine is produced in locus ceruleus of the pons
▪
Receptors A1, A2, B1, B2, and B3. More blood vessels.
▪
Fight or flight. Sympathetic nervous system.
▪
Concentrating, focusing, burst of energy, increased
BP/HR, mobilizing glucose
o
Epinephrine produced by the adrenal glands
▪
More heart
▪
Fight or flight. Sympathetic nervous system.
o
Acetylcholine synthesized by the Basal Nucleus of Meynart
▪
Parasympathetic Nervous system. Rest and Digest. Feed
and breed.