


Economic
Research
Service
Economic
Research
Report
Number 287
April 2021
The Opioid Epidemic: A Geography
in Two Phases
David A. McGranahan and Timothy S. Parker







































Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
An analysis of the relationship between physical disability rates and drug overdose mortality in rural areas during the opioid epidemic. The study uses data from 2000 to 2018 and finds that physical disability was a significant predictor of drug overdose mortality during the prescription phase of the epidemic. However, during the illicit phase, the association between physical disability and drug overdose mortality largely disintegrated. The document also discusses the role of population density and urban changes in drug mortality in the Northeast.
Typology: Exams
1 / 48

This page cannot be seen from the preview
Don't miss anything!
Economic Research Service
Economic Research Report Number 287
April 2021
Recommended citation format for this publication:
McGranahan, David A. and Timothy S. Parker. April 2021. The Opioid Epidemic: A Geography in Two Phases ERR-287, U.S. Department of Agriculture, Economic Research Service.
Cover photo images from Getty Images.
Use of commercial and trade names does not imply approval or constitute endorsement by USDA.
To ensure the quality of its research reports and satisfy governmentwide standards, ERS requires that all research reports with substantively new material be reviewed by qualified technical research peers. This technical peer review process, coordinated by ERS' Peer Review Coordinating Council, allows experts who possess the technical background, perspective, and expertise to provide an objective and meaningful assessment of the output’s substantive content and clarity of communication during the publication’s review.
In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering USDA programs are prohibited from discriminating based on race, color, national origin, religion, sex, gender identity (including gender expression), sexual orientation, disability, age, marital status, family/parental status, income derived from a public assistance program, political beliefs, or reprisal or retaliation for prior civil rights activity, in any program or activity conducted or funded by USDA (not all bases apply to all programs). Remedies and complaint filing deadlines vary by program or incident.
Persons with disabilities who require alternative means of communication for program information (e.g., Braille, large print, audiotape, American Sign Language, etc.) should contact the responsible Agency or USDA's TARGET Center at (202) 720-2600 (voice and TTY) or contact USDA through the Federal Relay Service at (800) 877-8339. Additionally, program infor- mation may be made available in languages other than English.
To file a program discrimination complaint, complete the USDA Program Discrimination Complaint Form, AD-3027, found online at How to File a Program Discrimination Complaint and at any USDA office or write a letter addressed to USDA and provide in the letter all of the information requested in the form. To request a copy of the complaint form, call (866) 632-9992. Submit your completed form or letter to USDA by: (1) mail: U.S. Department of Agriculture, Office of the Assistant Secretary for Civil Rights, 1400 Independence Avenue, SW, Washington, D.C. 20250-9410; (2) fax: (202) 690-7442; or (3) email: program. [email protected].
USDA is an equal opportunity provider, employer, and lender.
ii The Opioid Epidemic: A Geography in Two Phases, ERR-
Summary iii
Introduction 1
Physical Disability and the Rural Prescription Opioid Epidemic 6
Is our physical disability measure valid?............................................. Further evidence of the validity of our physical disability measure......................... Regional concentration of illicit opioid mortality..................................... 11
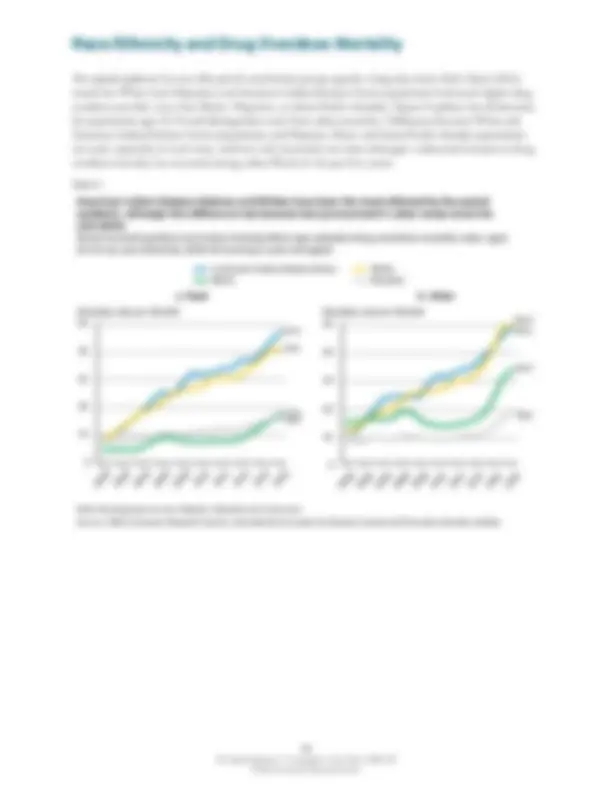
Race/Ethnicity and Drug Overdose Mortality 15
Multivariate Analyses of County Changes in White Drug Overdose Mortality: Prescription and Illicit Opioid Phases 20
Multivariate results............................................................ Employment change and drug overdose mortality in the illicit phase of the opioid epidemic: another look.........................................................
Conclusions 30
References 32
Appendix 1: Supplemental Analysis of County Adult Physical Disability Rate 36
Appendix 2: County Analyses of Drug Overdose Mortality in the Northeast and Remaining States: Means and Standard Deviations 42
ERS is a primary source of economic research and analysis from the U.S. Department of Agriculture, providing timely information on economic and policy issues related to agriculture, food, the environment, and rural America.
What Is the Issue?
Since the late 1990s, an opioid epidemic has afflicted the U.S. population, particularly people in prime working ages of 25-54. Driven by the opioid epidemic, the age-adjusted overall mortality rate from drug overdoses rose from 6.1 per 100,000 people in 1999 to 21.7 per 100,000 in 2017, before dropping to 20.7 per 100,000 in 2018. The drug overdose mortality rate among the prime working age population was 36.5 deaths per 100,000 people in 2018. Among major causes of death in this population, this rate was exceeded only by cancer (40.5 deaths per 100,000) in
What caused this epidemic, and who has been most affected? One view is that economic misfor- tune has driven many working-age people to self-destructive behavior—marked by increasing drug and alcohol abuse and suicide. However, another line of research shows that local economic downturns have been a small factor in the geography of the drug overdose epidemic. A second view faults the widespread introduction of new opioid prescription painkillers, succeeded in recent years by the spread of heroin and powerful synthetics such as fentanyl. This view, which has received less research attention, is the focus of this study.
What Did the Study Find?
The study found evidence that the introduction and supply of new opioid drugs, whether through prescription painkillers in the 2000s or illicit opioids such as fentanyl in the 2010s, were major drivers of the opioid epidemic. These two drivers involved such different demographic groups and geographic areas that, in many ways, they comprise distinct phases of the epidemic. Mortality data indicate that the earlier “prescription opioid phase,” from about 2000 to 2011, most affected adults in the age range of 25-54, Native American/Alaskan Natives and Whites, and rural more than urban populations. In this phase, the epidemic was most severe in areas of high physical disability rates, which, following epidemiological research, we use as an indicator of physical pain. We found little evidence that local economic misfortune accounted for the substantial geographic differences in the severity of this phase across State rural areas or counties.
1 The Opioid Epidemic: A Geography in Two Phases, ERR-
In 2011, a Centers for Disease Control and Prevention (CDC) report labeled the high and rising mortality from prescription opioid overdoses a national epidemic (Paolozzi et al., 2011). The epidemic was largely responsible for doubling the number of drug overdose deaths nationwide, from 17,000 in 2000 to 36,000 in
2007.^1 The drug overdose epidemic has since surged, with the number of drug overdose deaths redoubling to more than 70,000 by 2017 before falling to 67,000 in 2018.^2 ,^3
Although drug abuse historically has been largely an urban problem, rural areas have been drawn into the opioid epidemic (Mack et al., 2017). According to a 2018 survey, rural Americans identify drug addiction or abuse (including opioids) and economic concerns as the two biggest problems facing their local communities (National Public Radio/Robert Wood Johnson Foundation/Harvard T.H. Chan School of Public Health, p.1). Indeed, throughout the 2000s, rural (nonmetropolitan) drug overdose mortality rates rose faster than urban (metropolitan) rates and exceeded urban rates by the end of the decade (figure 1).^4 While rural rates continued to rise in the 2010s, the urban rates jumped even more. The central purpose of this study is to better understand the geography and demography of the opioid epidemic, particularly as it has spread into rural areas.
Figure 1
(^1) Numbers downloaded from the Centers for Disease Control and Prevention Wonder website. (^2) To add perspective, deaths from firearms in the United States rose by 38 percent between 2000 and 2017 to a total of 39,000. (^3) Provisional national estimates for 2019 indicate that drug overdose mortality rose again in 2019, edging above the 2017 rate. A recent American Medical Association news brief cited a wide range of news sources suggesting the COVID-19 pandemic aggravated the opioid epidemic in 2020 by drawing away health resources, isolating addicts, and increasing unemployment, creating situations to drug abuse. The spread of fentanyl and its analogs out of the Northeast is likely adding to the fire. (^4) Throughout this report, we include drug overdose mortality from accidents, suicide, assault (intentional poisoning of another person), and unknown intent in our measure of drug overdose deaths.
0
5
10
15
20
25
Deaths per 100,
Year
Rural Urban
Between 1999 and 2011, rural growth in drug mortality exceeded urban Rural and urban age-adjusted drug overdose mortality rates, 1999-
Note: Rural is equivalent to nonmetropolitan in 2013, while urban is metropolitan. Source: USDA, Economic Research Service using data from the Centers for Disease Control and Prevention Wonder website.
19992000200120022003200420052006200720082009201020112012201320142015201620172018
2 The Opioid Epidemic: A Geography in Two Phases, ERR-
There are basically two schools of thought about the rise in drug overdose mortality. One emphasizes drug supply, which involves an increased availability of licit drugs through the introduction and prescription of new opioid painkillers in the late 1990s and 2000s. This was encouraged by a growing belief in the medical community that pain should be treated independently of its cause and that treatment with narcotics rarely developed into addiction (Quinones, 2015).^5 From this perspective, the geography of the rise in drug over- dose deaths in the 2000s should mirror the geography of pain. However, while there has been research on the geography of prescriptions (e.g., McDonald et al., 2012; Paolozzi et al., 2014), the role of pain in this geog- raphy—or the geography of drug overdose mortality—has not been explored. An exception is a small English study that drew on the Health Survey of England for measures of pain and found regional differences in pain associated with variation in opioid analgesic use (Todd et al., 2018).
The second school of thought has focused on shrinking local economic opportunities that may increase people’s tendency to use drugs as a relief from mental stress. Case and Deaton (2015) noted the simulta- neous rise in deaths from suicide, alcohol poisoning, and drug overdoses, particularly among midlife Whites without a college degree. Case and Deaton (2017) conjectured that the declining fortunes of Whites who had been middleclass led to an increase in what they called “deaths of despair.” From this perspective, drug mortality among middle-aged Whites rose because of an increase in demand for emotional painkillers.
The idea that unhealthful behavior rises in times of economic stress is not new. A recent international survey of published research on the effects of recession and unemployment on illegal drug use found broad evidence for this link (Nagelhout et al., 2017). Studies following Case and Deaton (2015) provided some support with respect to the influence of trade with China in the disappearance of manufacturing jobs (Pierce and Schott, 2016; Autor et al., 2018). In related results, Betz and Jones (2018) found that employment effects on county changes in opioid deaths were stronger when the analysis focused on industries likely to employ less-skilled workers. In a study of manufacturing counties between 1999 and 2016, counties exposed to auto manufac- turing plant closures had greater increases in opioid deaths per 100,000 working-age people in the subse- quent 5 years than over the same period among manufacturing counties not exposed to auto plant closures (Venkataramani et al., 2019).
It is easy to slip from the finding that economic misfortunes resulted in a rise in drug overdose mortality to an assumption that the opioid epidemic could be explained by a rise in despair. However, in a careful analysis including many of the same trade and industry measures analyzed in the above studies, Ruhm (2019) found that economic misfortune has played, at best, a small role in the drug overdose epidemic. This finding reso- nated with Betz and Jones (2018), who noted that their own analysis did little to explain why the epidemic affected some localities so much more than others since 2000. In addition, a series of studies by Shannon Monnat of the relationships between demographic, socioeconomic, and other factors with drug overdose mortality and mortality from specific opioids made clear that the antecedents to the opioid epidemic include social and economic factors that go well beyond the loss of manufacturing jobs (Monnat, 2018; Monnat, 2019; and Monnat et al., 2019). Finally, Case and Deaton (2017) raised questions about a direct link between the recessions in the post-2000 period and the spike in drug overdose mortality—suggesting a longer, even multigenerational, gestation.^6
In the sharpest challenge to the “deaths of despair” story of the opioid epidemic, Ruhm (2019) noted changes in the demographic characteristics of opioid overdose mortality in the early 2010s as prescription opioids became less available and drugs such as fentanyl and heroin became more available. In this study, we examine
(^5) Other investigative reporters (e.g., McGreal, 2018; Macy, 2018; Meier, 2018) looking into the development of the opioid epidemic also emphasized new and heavily marketed opioid drugs and greater emphasis on pain reduction in the medical community as contrib- uting factors during this period. (^6) Most recently, Case and Deaton (2020) focused on the long-term decline in the economic well-being of midlife Whites without a college degree.
4 The Opioid Epidemic: A Geography in Two Phases, ERR-
In some situations, these illicit drugs may be replacing and supplementing prescription opioids,^8 but, as noted by Ruhm (2019), the demography of the epidemic changed as illicit opioids became more widely used. During the prescription opioid phase, drug-overdose mortality increased most among middle-aged men and women in both rural and urban areas, but more recently young men (ages 25-39) seem the most affected (figure 3). Moreover, it seems likely the sale of illicit opioids faces different contingencies than prescription opioids. For instance, because these new illicit opioids are less targeted toward pain relief, their geography and associated mortality may be more reflective of local economic misfortune than are prescription opioids. Also, without reliance on local pharmacies for distribution, sales networks may be thin in rural areas, especially those that are sparsely settled.
The study considers heroin and synthetic opioids such as fentanyl to be “illicit opioids,” since they track roughly the same demography and geography. However, their roles in the opioid epidemic have been quite different. Heroin generally serves as an alternative to other drugs, including prescription opioids.^5 In contrast, illicit fentanyl and its analogs more often serve as high-strength supplements, mixed with and adding to the effects of heroin, cocaine, prescription opioids, or other addictive drugs (Hedegaard et al., 2008). More than creating new addictions, fentanyl and its analogs have likely made existing addictions more lethal.
Figure 3
(^8) Evans et al. (2019) found that the 2010 reformulation of time-release OxyContin, which made it impossible to release all the medi- cation at once, “ignited the heroin epidemic” as people switched to more accessible drugs.
After 2010-12, the rise in drug overdose mortality involved primarily young adult males Drug overdose mortality rates by rural-urban (nonmetropolitan-metropolitan) location, sex, and age group, 1999-2002, 2010-12, and 2016-18 averages Rural
Urban
Mortality per 100,
Rural Mortality per 100,
Mortality per 100,
Urban Mortality per 100,
0
10
20
30
40
50
60
10-1415-1920-2425-2930-3435-3940-4445-4950-5455-5960-6465-6970-7475-7980-
Female
0
10
20
30
40
50
60
10-1415-1920-2425-2930-3435-3940-4445-4950-5455-5960-6465-6970-7475-7980-
Male
0
10
20
30
40
50
60
10-1415-1920-2425-2930-3435-3940-4445-4950-5455-5960-6465-6970-7475-7980- Age group
0
10
20
30
40
50
60
10-1415-1920-2425-2930-3435-3940-4445-4950-5455-5960-6465-6970-7475-7980- Age group
Age group Age group
Male
Source: USDA, Economic Research Service calculations using Centers for Disease Control and Prevention Wonder data.
Figure 3a Figure 3b
Figure 3c Figure 3d
2016- 2010- 1999-
2016- 2010- 1999-
2016- 2010- 1999-
2016- 2010- 1999-
Female
5 The Opioid Epidemic: A Geography in Two Phases, ERR-
Previous research on the changing geography of opioids since 1999 has treated that time as a single period. The central thesis of this study is that drug overdose mortality in the prescription opioid and illicit opioid phases had different drivers and different geographies. Prescription opioids and resulting mortality were highest in counties with high incidences of physical disability, while illicit opioids went to more densely settled counties in the Northeast, particularly those with limited economic opportunities for young adults.
The study presents three distinct analyses related to the drug epidemic, each with its own section. The first focuses on physical disability as the driver of the spread of prescription opioids and drug overdose mortality in the 2000s and its subsequent ebbing influence on the opioid epidemic’s geography as the illicit opioid phase became predominant. This analysis focuses on areas outside metropolitan boundaries, labeled “State rural areas.” The second analysis focuses on the distinct experiences of different racial/ethnic groups, as the opioid epidemic has not been pandemic across all groups. The third analysis uses county data to consider community factors (such as local education levels and employment change) that may have affected the epidemic’s geography during each phase.
Opioid prescription data
Yearly estimates of the number of county retail opioid prescriptions per capita were downloaded from the Centers for Disease Control and Prevention for 2006 to 2017 on its website under “drug overdose maps.” The data are not available by age, race/ethnicity, or any other population subgroup. We present data for 2010-12, the 3 years with the largest number of prescriptions, recalculating rates from per 100 residents to per 100 residents ages 25 to 54, surmising from mortality rates that this is the population most likely to have received retail prescriptions (see figure 3). The data are from pharmacy records that provide the pharmacy location but not recipient residences. During this period, approximately 13 percent of the coun- ties had no records because the county had no pharmacy, none was sampled, or the data were erroneously attributed to an adjacent, more populous county according to the sampling rules used. There are obvious questions about the validity of the data for smaller rural counties. Analyzing State rural areas rather than counties largely avoids these problems but at the expense of having a small number of cases (47) and elimi- nating within-State differences from the analysis.
7 The Opioid Epidemic: A Geography in Two Phases, ERR-
Further evidence of the validity of our physical disability measure
Despite using a measure from the population census rather than administrative records and using a gauge from a time of prosperity, continued skepticism among some researchers led us to undertake two analyses to test the validity of physical disability as a measure of chronic pain.
The first analysis examined two issues: whether physical disability was negatively associated with prior employment change, and whether the measure was sensitive to conditions known to be associated with chronic disease. Here we drew on the “life course” approach to health problems, which has shown that difficult experiences in childhood tend to be associated with health problems later in life (Case et al., 2005; Montez and Hayward, 2014; Monnat and Chandler, 2015). The closest precedent to our analysis is Bowen and Gonzalez (2010), who used survey data from older Americans to show that childhood socioeconomic stress had a bearing on chronic disabilities in adulthood, even when taking respondents’ present-day socioeco- nomic situations into account.
Using child poverty rates in 1970 to reflect county socioeconomic stress when the current middle-age popula- tion was young, we found this stress correlated with local adult physical disability (ages 21-64) rates in 2000, even when considering current adult poverty (see Appendix 1 and its table 1.2). Further, self-reported physical disability in the working-age population in 2000 was not related to employment change over the previous decade as skeptics of physical disability measures have suggested, perhaps because the U.S. economy was rela- tively healthy in the 1990s.
The second analysis related to physical disability outcomes. To the extent that our measure reflects the perva- siveness of chronic disease, counties with high physical disability rates should also have high mortality rates from natural causes (defined here to include all deaths except those related to accidents, suicide, or homi- cide), other conditions being equal. Even after taking into account local education—a strong predictor of health (Cutler and Lleras-Muney, 2011) and longevity (Lleras-Muney, 2005)—and the deleterious effects of poverty (Adler and Stewart, 2010), we found across State rural areas that 2000 physical disability rates among Whites (ages 21-64) were strongly related to their natural cause mortality rates in 1999-2002 (appendix table 1.3). We obtained similar results when we repeated the analysis for rural counties alone and for all counties, confirming their robustness.
These analyses together support the validity of our physical disability measure and suggest that residents of counties with high levels of reported physical disability were likely target populations for prescription opioids.
State rural area physical disability, opioid prescriptions, and drug overdose
mortality
The tie between physical disability and opioid prescriptions is remarkably strong. Physical disability in the rural (nonmetropolitan) population ages 21-64 in 2000 accounted for a substantial 71 percent of the variance in opioid prescriptions across State rural areas 10-12 years later (figure 4).^11 Rural Kentucky, West Virginia, and Tennessee had the highest physical disability rates—and the highest opioid prescription rates in 2010-12. Heavily agricultural States, including the Dakotas, Iowa, Minnesota, and Nebraska, had among the lowest physical disability rates and correspondingly relatively few prescriptions per prime-age adult.
(^11) Variance here is a statistical term denoting differences across units, in this case State rural areas. If physical disability allowed us to predict county drug prescriptions exactly, it would account for 100 percent of the variance in prescription rates across counties. At the other extreme, if physical disability was absolutely no help in predicting county prescription rates, the variance accounted for would be zero. As evident in the scatter plot, physical disability is a good predictor of State rural area prescription rates.
8 The Opioid Epidemic: A Geography in Two Phases, ERR-
Figure 4
Affirming the relevance of physical disability, the socioeconomic measures in this study (also from Census
5.0 7.5 10.0 12.5 15.
500
400
300
200
100
0
WI
WV
WA
VA
VT
UT (^) TX
TN
SD
SC
PA
OR
OK
OH
ND
NC
NY
NM
NH
NV
NE MT
MO
MS
MN
MI
MA
MD ME
LA
KY
KS
IA
IN IL
HIID
GA FL
CT
CO
CA
AR
AZ
AK
AL
Rural county opioid retail prescription rates in 2010-12 were closely tied to 2000 physical disability rates Physical disability rate, ages 21-64, 2000, and average annual retail opioid prescription rates per 100 residents ages 25-54, 2010-12, by State rural (nonmetropolitan) area
Variance accounted for: 71 percent
Note: The line and its variance accounted for are derived from regression analysis. The “variance accounted for” measures how close the dots are to the line and ranges from zero percent (no association) to 100 percent (perfect fit). Source: USDA, Economic Research Service calculations using data from the Centers for Disease Control and Preven- tion and U.S. Census Bureau.
Annual average opioid retail prescriptions per 100 residents, ages 25- 54 (2010-12)
Percent reporting physical disability, ages 21-64 (2000)
10 The Opioid Epidemic: A Geography in Two Phases, ERR-
Figure 5^ Drug overdose mortality was most closely associated with physical disability at the peak of the opioid prescription phase in 2010-12^ State rural (nonmetropolitan) area physical disability, ages 21-64, 2000 and age-adjusted drug overdose mortality rates, ages 25-54, at three stages of theopioid epidemic^ Note: Physical disability is for ages 16-64. Sloped lines and variances accounted for derive from regression analyses. The variance accounted for is a measure of how close the dots are to thelines and varies from 0 to 100 percent, when the dots are all on the line. The orange dots represent the top 9 States in gains in rural drug overdose mortality between 2010-12 and 2016-18: CT,ME, MD, MA, NH, NY, OH, PA, and VT.Source: USDA, Economic Research Service calculations using the Centers for Disease Control and Prevention Wonder and U.S. Census Bureau data.
Percent reporting physical disability, ages 21-64, 2000
80 70 60 50 40 30 20 10 0
WY
WI
WV
WA
VA
UT VT
TX
TN
SC
OR
OK
ND
NC NY
NM
NH
NV
NE
MT
MSMO
MN
MI
MA
MD
ME
LA
KY
KS IA
IN (^) IL ID HI
GA
FL
CT
CO
CA
AR
AZ
AK
AL
80 70 60 50 40 30 20 10 0
VT
OHPA NY
NH
MA
MD
ME
WYCT
WI
WV
WA
VA
UT
TX
TN
SD
OK ORSC
ND
NM NC NV
NE
MT
MO MS
MN
MI
LA
KY
KS
IA
IN
ILID HI
GA
FL
CO
CA
AR
AZ
AL
80 70 60 50 40 30 20 10 0
VT
OH PA
NY
NH MA
MD
ME
CT WI WY
WV
WA
VA
UT
TX
TN
SD
SC OR
OK
ND
NC NM NV
NE
MT
MO
MS
MN
MI
LA
KY
KS IA
IN IL
ID HI
GA
FL
CO
CA
AR
AZ
AK
AL
a. Start of prescription phase (1999-2002)
b. Peak of prescription phase, beginning of illicit
opioid phase (2010-12)
c. Study peak of Illicit opioid phase (2016-18)
Variance accounted for: 19 percent
Variance accounted for: 46 percent
Variance accounted for: 4 percent
Mortality rate per 100,
Mortality rate per 100,
Mortality rate per 100,
11 The Opioid Epidemic: A Geography in Two Phases, ERR-
Drug overdose mortality in State rural areas
Any analysis of the opioid mortality epidemic faces unfortunate tradeoffs as to the choice of a measure to use. Data on opioid overdose mortality alone are available but incomplete. Although records are improving, those filling out death certificates are not required and are not necessarily able to identify drugs involved in overdose deaths and often do not; consequently, actual deaths from opioids are under- estimated (Ruhm, 2019). The degree of underestimation varies geographically. The broader alternative measure, drug overdose mortality, results from a variety of drugs besides opioids, such as methamphet- amines or cocaine, so using drug overdose mortality as a proxy for opioid deaths results in some overesti- mating of the role of opioids. Overestimation likely would vary from place to place, depending on what other drugs are in use.
Using 2010-12 data for State rural areas, we found that the opioid prescription measure accounted for a much higher proportion of the variation in drug overdose mortality overall (40 percent) than in drug overdose mortality specifically from opioids (23 percent). Similar results were obtained for physical disability in individuals ages 21-64: 48 percent versus 33 percent. This pattern suggests that, despite the inclusion of other drugs, drug overdose mortality better reflects the opioid crisis than the opioid death measure, for which data are missing. We assume these biases have remained constant and use the opioid mortality measures only to compare trends in different types of opioids, figures 2 and 6 being examples.
Regional concentration of illicit opioid mortality
This association between areas of physical disability and rises in drug overdose mortality largely disintegrated by 2016-18. For many State rural areas, there was little change in drug overdose mortality rates between 2010-12 and 2016-18. However, for nine State rural areas in the Northeast quadrant of the United States, the rate rose by more than 20 and sometimes 30 deaths per 100,000: Connecticut (CT), Maine (ME), Maryland (MD), Massachusetts (MA), New Hampshire (NH), New York (NY), Ohio (OH), Pennsylvania (PA), and Vermont (VT).^14 These rural areas, indicated by red markers in figures 5b and 5c, do not have particularly high rates of physical disability, but in 2016-18 they were among the areas with the highest rates of drug over- dose mortality.
Mortality associated with heroin and synthetic opioids such as fentanyl increased at an extraordinary pace between 2010-12 and 2016-18 in these nine rural areas, especially among young adults (ages 25 to 39) (figure 6a).^15 Mortality from these drugs also increased in the rural parts of other States, but generally at more modest paces among both young and middle-aged adults (figure 6b).
(^14) We use the term “northeastern quadrant” or “Northeast” to designate this group of States, later including completely urban States: Delaware (DE) New Jersey (NJ), and Rhode Island (RI), and the District of Columbia (DC), which are contiguous. This desig- nation should not be confused with the Census-defined Northeast Region, which does not include OH, MD, or DC. (^15) Improved detail on death certificates of the particular drugs involved in fatal drug overdoses may have somewhat exaggerated the rise in deaths from fentanyl-type drugs and understated the decline in other drugs over the study period. Hedegaard et al. (2018) reported that the proportion of drug overdose deaths that did not mention a particular drug or drug class declined from 22 percent in 2011 to 13 percent in 2016.
13 The Opioid Epidemic: A Geography in Two Phases, ERR-
Figure 7
Changes in rural drug overdose mortality became tied to population density in the illicit opioid phase State rural (nonmetropolitan) area population density and changes in age-adjusted drug overdose mortality rates, ages 25-
Note: The orange dots indicate State rural areas ranked in the top 9 for gain in drug-overdose mortality, 2010-12 to 2016-18 (CT, ME, MD, MA, NH, NY, OH, PA, and VT). Sloped lines and variances accounted for are derived from regressions. Variance accounted for is a measure of the distance of the dots from the line, and ranges from 0, when the dots do not follow a line at all, to 100 percent, when the dots are all exactly on the line. Source: USDA, Economic Research Service calculations using data from the Centers for Disease Control and Prevention and U.S. Census Bureau.
Change in mortality rate per 100,000 Change in mortality rate per 100,
Population per square mile of land area, 2000
0 50 100 150 200
60
50
40
30
20
10
0
VT (^) PA
OH
NY
NH
MA
ME MD
CT
WY
WI
WA
VA UT TN
SD SC
OR
OK
ND (^) NC
NM
NV
NE MT
MO MS
MN MI
LA
KY
IA
IN IL
ID
HI GA
CO FL
CA
AR
AZ AK AL
0 50 100 150 200
60
50
40
30
20
10
0
VT
PA OH
NY NH
MA
MD ME CT
WY
WI
WV
WA
VA UT
TX
TN
SD
SC OR
OK
ND
NM NC
NV
NE
MT
MO
MNMS
LA
KY
KS IA
IN IL ID
HI
CO FLGA
CA AR
AKAZ
AL
Variance accounted for 1 percent
Variance accounted for 44 percent
a. Prescription phase, 1999-2002 to 2010-12 b. Illicit opioid phase, 2010-12 to 2016-
The State rural areas of high gain in drug overdose mortality in the Northeast tended to have higher residen- tial density (r=0.51) and higher urban increases in drug overdose mortality than other States (r=0.66). Do these qualities account for the very high increases in drug overdose mortality in the rural Northeast quadrant between 2010-12 and 2016-18, or are there other drivers? Table 1 reports the results of a multivariate anal- ysis of the associations of these measures with changes in rural drug overdose mortality in the 2010s. Also included was the rural physical disability rate on the expectation that, because of restrictions on prescriptions and changes in the formulation of the opioid Oxycontin, disability might be associated with declines in drug overdose mortality in this period.
From equation 1 in table 1 it is apparent that all three factors—lower rates of physical disability, urban gain in drug overdose mortality, and population density—help account for the changing geography in the rural drug overdose epidemic in 2010-12 and 2016-18. When we also consider the nine Northeast States with the highest rural gains in drug overdose mortality as a group, however (equation 2), it is apparent that these three
14 The Opioid Epidemic: A Geography in Two Phases, ERR-
factors do not fully account for the greater gains in these States: The sizable partial correlation of being in a northeastern State with change in mortality (rp= 0.67) indicates an independent relationship.^16
Table 1 Population density and State urban changes in drug mortality account for only some of the substantial increases in State rural area drug mortality in the Northeast in 2010-12 to 2016- Regression of changes in age-adjusted State rural (nonmetropolitan) area drug overdose mortality rates, ages 25-54, 2010-12 to 2016-18 on selected area characteristics
Coefficients Equation 1 Equation 2 Area attributes r Partial r Partial r Physical disability rate, 2000 -0.37 -0.69 -0. Change in State urban drug overdose mortality, 2010-12 to 2015-17, ages 25-
0.71 0.69 0.
Population density, 2000 0.67 0.37 0. Northeast State 0.88 0.
R^2 (percent of variation accounted for) 76 87 N=
Note: Coefficients are all statistically significant (p<.05 level). Northeast States with rural areas include CT, ME, MD, MA, NH, NY, OH, PA, and VT. Physical disability is for ages 21-64. r = correlation coefficient. Partial r = partial correlation coefficient.
Source: USDA, Economic Research Service, calculations based on data from Centers for Disease Control and Prevention Wonder website and the U.S. Census Bureau.
Regional concentration seems then to be a separate factor shaping the geography of the rise in illicit drug mortality. Not only were all nine States with high rural gains in the northeastern quadrant of the United States (see figure 7b), the 14 States with the highest urban area gains include all but one of the nine top States in rural gains and the completely urban (by our definition) neighboring States of Delaware (DE), New Jersey (NJ), and Rhode Island (RI), and the District of Columbia.17 18^ This centering on the northeastern quadrant seems likely to be at least partly the result of drug ports of entry and contagion, where problems leak across State lines.
The analysis in this section has looked at the changing geography of the rural drug epidemic using State rural areas as the units of comparison. In section C below, we address some of the same questions using counties as units of comparison. That analysis allows greater attention to the role of local economic hardship in the geog- raphy of the drug epidemic within the Northeast.
(^16) A comparison of the correlations in this table with comparable correlation statistics for 1999-2002 to 2010-12 demonstrates the sharp differences in the geographies of change in drug overdose mortality between the two periods. Thus, the correlation of physical disability with change in drug overdose mortality went from r= 0.65 in the 2000s to r=-0.37 in the 2010s. On the other hand, corre- lations involving urban drug overdose mortality (r=0.33), population density (r=0.11), and Northeast location (r=-0.07) were much smaller in the 2000s than in the 2010s. (^17) Kentucky and West Virginia were exceptions, with high urban gains, but perhaps because of low rural population density and isolation from urban areas, very low (West Virginia) or nonexistent (Kentucky) rural gains. (^18) For another analysis of regional concentration, based on drug mortality levels rather than change but highlighting different types of drugs, see Kiang et al., 2019.