Download USMLE Multi-Systemic Pathophysiology 2025/2026: Linking Normal Function to Disease and more Exams Medicine in PDF only on Docsity!
Item: 1 of S - , • Mark - "'I^ ~^ ··^ ~
QIO: 3134 ~^ P~v•ous^ N@xt^ Lab^ l lues^ Notes^ Calculator
. 1
· 3
· 5
A newly marri ed couple is frustrat ed wit h the ir inabilit y to conceive a^ child.^ They make^ an^ appoin^ tme^ nt^ at^ a^ fertility^ clinic,^ where the 28-^ ~~AI year-old^ man^ is^ diagnosed witha^ low^ sperm count wit h no apparent cause. Repeated^ attempts^ at in vitro^ fertilizat ion^ are^ unsuccessful.^ At their next clinic appoi ntment,^ the^ man inquires about an^ alternative^ method^ for^ improving^ fertility^ t hat he discovered on^ the^ Internet.^ The physician has never used clomiphene ci trate^ for^ male^ infertility^ before and decides to research its modeofact ion.
Ifthe patient were to take clomiphene citrate, whichofthe^ following^ hormone receptors^ would^ most^ likely^ be affected?
: A. Estrogen
B. Gonadotropin-releasing hormone
C. Inhibin
D. Luteinizing hormone
E. Testosterone
8 s^^8 Lode. Suspe-nd^ E^ nd^ Bloc:k
Item: 1 of S ~ , • Mark <::J [:::> "" I ~ · ~'j QID: 3134 J.. Previous Next LAb faiUI~S Notes Calculator 1
T he co rr ec t a ns we r is A. 3 6°/o ch ose t h is.
Clomiphene cit rat e is a select ive est rogen rece ptor modulat or (SERM) t hat works as an ant iest rogen at t he level of t he hypot halamus, reducing t he feedback inhi bi t ion effect of est rogen. This leads to increased secret ion of gonad ot ropi n- releasing hormone (GnRH) from the hypothalamus, which ult imate ly leads t o increased secretion of follicle-st imulat ing hormone (FSH) and luteinizing hormo ne (LH) from t he pi tu itary. LH increases test ostero ne pr oduct ion in the Leydig ce lls, which in some men results in increased f ert ility. Clomiphene fo r male hypogonadism is an off-label use, but it has been proven t o be a more desirable t reat ment than test osterone replacement therapy. Clomiphene is more commo n ly used f or fema le infe rt ility, pa rt icularl y in anov u lat ion seen in pol ycyst ic ovari an sy ndrome. Follicle-stimulating hormone Selective estrogen receptor modulator Antiestrogen Luteinizing hormone Off-label use Gonadotropin-releasing hormone Anovulation Polycystic ovary syndrome Hypothalamus Estrogen Estrogen receptor Testosterone Clomifene Hypogonadism Androgen replacement therapy Hormone Pituitary gland Leydig cell Female infertility Infertility Enzyme inhibitor Receptor (biochemistry) Citric acid
B is not co rr ect. 28% c ho se thi s.
GnRH is key to the fe rt ili ty benefit of clomiphene cit rat e, but estrogen signaling is most direct ly affected. Secr et ion of GnRH from the hypothalamus increases as a result of reduced feedback inhi bi t ion by est rogen. Estrogen Hypothalamus Clomifene Gonadotropin-releasing hormone Enzyme inhibitor Citric acid Fertility
C is not cor r ect. 8 °/o c ho se thi s.
I nhi bi n is produ ce d by t he Sertoli cells in response to follicle -st imulat ing (FSH). It acts as negative feedback at the an terior pi tu itary f or FS H secret ion, thereby decreasing spermatogenesis. Spermatogenesis Anterior pituitary Activin and inhibin Sertoli cell Pituitary gland Negative feedback Follicle-stimulating hormone Anatomical terms of location
D is not co r rect. 1 8% c h ose th is.
Although lut einizing hormone act s on the Leydig cells of t he t estes to st imulat e t estost erone synthesis, which is key t o im pr oveme nt in fe rt ilit y, clomiphene cit rat e acts most direct ly on est rogen. Luteinizing hormone Testosterone Estrogen Clomifene Testicle Hormone Leydig cell Citric acid
E is not co rr ec t. 1 0°/o ch ose thi s.
Test ost erone is t he end product of clomiphene cit rate, but est rogen signaling is most direct ly affected by cl omiphe ne cit ra te dosing. Estrogen Testosterone Clomifene Citric acid
8 s 0 Lock Suspend End Block
Item: 2 of S - , • Mark - "'I^ ~^ ··^ ~
QIO: 3133 ~^ P~v•ous^ N@xt^ Lab^ l lues^ Notes^ Calculator
1
· 3
· 5
A 4 3- year-old man com es into the office complain in g of a rec ed ing hairline in the frontas^ well^ as^ thinning of his hair at^ the^ crown. The man^ ~~AI stat^ es^ thathis father's hairis dist ri^ bu^ t^ ed^ in a horseshoe pattern. The physician specul^ at^ es^ t hathis condit ion^ may^ be^ due to a particular hormone t h at is present in higher^ levels^ and decides t o prescribe a drug t h^ at^ inhibit s it s pro^ du^ ct ion.
Whi chofthe fol lowing enzy m es is inhibited by^ t he drug m^ os^ t^ likely^ prescribed?
: A. 21o-Hydroxylase
B. So-Reductase
C. 5'-Deiodinase
D. Aromatase
E. Desmolase
8 s^^8 Lode. Suspe-nd^ E^ nd^ Bloc:k
Item: 2 of S ~ , • Mark <::J [:::> "" I ~ · ~'j
QID: 3133 J.. Previous Next LAb faiUI~S Notes Calculator
1 2
T he co rr ec t a n swe r is B. 77% ch ose t his.
Ma le- patt ern baldness is relat ed to the presen ce of dihydrotestosterone (DHT). Test osterone is convert ed to DH T by the enzyme Sa -reductase. It is believed that elevated levels of DHT "burn out " t he hair follicle, causing t he follicle t o slow down production, producing hair t hat is weaker and sho rt er. Therefor e, it is thought that decreasing the product ion of DH T reduces hair loss. Sa - Red uctase inhibi to rs (eg, finast eride) are also used t o t reat mild- to -mode ra t e benign pr ostat ic hyperplasia. Pa t ients wit h congenital Sa -reductase def iciency are usually genet ically ma l e, as DHT has no defined role in fe male development. This def iciency presents in infant s wi th am biguous genitalia (usually m icropenis or macro cl itoris); although t est icles are usually present , t hese pat ien ts usually have female pri mary sex characte rist ics and are ra ised as girls. Du ri ng pubert y, when t estost erone levels ri se dramat ically, t he person begins t o develop male secondary sexual characte rist i cs , and the genitals are masculinized. Benign prostatic hyperplasia Hair follicle Finasteride Micropenis Dihydrotestosterone Male-pattern hair loss Testosterone Enzyme Ambiguous genitalia Sex organ Testicle Hair loss Puberty Secondary sex characteristic Clitoromegaly Hyperplasia OVarian follicle Congenital disorder Virilization Benign tumor
A is not corre ct. 6°/o ch ose thi s.
21a -Hydroxylase is responsible f or t he synt hesis of aldost erone and cort isol. Patien ts wi th 21a- hydroxylase def iciency experience congenita l adrenal hyperplasia, a condit ion characteriz ed by salt wast ing and viril izat ion in female pat ients. Virilization Cortisol Aldosterone Hyperplasia Congenital disorder
C is not co rr ec t. 3 °/o c ho se thi s.
S'-Deiodinase is req uired during t hyroid hormone sy nthesis for t he conversion of t hyr ox ine t o t ri iodot hyroni ne. Although t hyroid hormone deficiency may lead to br it t le hai r, a physician would not t reat male- pat tern baldness by prescri bi ng a drug to inhibit S' -deiodinase. S' - Deiodinase inhi bi tors such as propyl th iouraci l are used t o block t he pr oduct ion of tri i odothy ronine in hype rt hyroidism. Propylthiouracil Thyroid hormone Hyperthyroidism Triiodothyronine Hypothyroidism Thyroid Hormone Hair loss Physician
D is not co r re c t. 11 % c h ose th is.
Aromat ase is req uired fo r the synthesis of est rogen. I n male- pattern ba ldness, t he prob l em is n ot the presen ce of estrogen; ra t h e r~ it is the overproduct ion of t estost erone. Aromatase inhi bi tors are used to t reat breast cancer by blocking the synthesis of est rogen, t hus hindering t he growt h of est rogen -sen si t ive tu mo rs. Aromat ase i nh ibit ors are not used in t he t reatment of male- patt ern baldness. Testosterone Male-pattern hair loss Aromatase Estrogen Aromatase inhibitor Breast cancer Hair loss Cancer Neoplasm
E is not co rr ec t. 3°/o chos e thi s.
Desmolase con verts cholest erol in to pregnenolone. Pregnenolone ca n t hen be conve rt ed i nto m ineralocorticoids, co rt icosteroids, or sex hormones. Desmolase inhi bi tors would not be indi ca t ed for a pat ient wit h isolat ed male- pattern baldness. Pregnenolone Male-pattern hair loss Corticosteroid Mineralocorticoid Cholesterol side-chain cleavage enzyme Cholesterol Sex steroid Desmolase Hair loss
8 s 0 Lock Suspend End Block
Ite m : 2 o f S - , • Mark - "'I^ ~^ ··^ ~
QIO: 3133 ~^ P~v•ous^ N@xt^ Lab^ l^ lues^ Notes^ Calculator
1 2
· 3
· 5
FA17 p 318.1 •
Adrenal steroidsand^ congenital^ adrenal^ hyperplasias
ACTH Ketoconazole^ (blo^ •^ ;eve~^ .teps^ mstero1doo•nesisJ
CholesterOl lvlcl StAR> 1 ±-J
l
1 Anastrozole.^ exemestane
AngiotenSin II
Pregnenolone^ 17a-hydroxvt.>s£^ S^
17u otlydroxylase
l
17-hydroxypregnenolone^ 1:1^ l>ehydroep1androsterone^ (DHEA)
Progesterone ...:....:._:........:...~-+ """"'""""' 171 - hydroxyprogesterone 17a hydm Androstenedione - """"""===-+-~~
ll·deoxycort•costerone
I
Corticosterone
J Aldosterone
ZONA GLOMERULOSA
ll·deoxycortisol
Cortisol
li-E>- Glycyrrhetinic ac1d
Cortisone
ZONA FASCICULATA rJetrnrtvtvniAc
Testosterone Aromatase
Sa-reductase
ZONA^ RET1CULARIS ,,..,.,I'V'WN"t<.
Estrone
Estradiol
Dthydrotestosterone !DHT}
Finastende
.Wtfflftall NJT __ ....J
8 s^8
Lode. Suspe-nd^ E^ nd^ Bloc:k
· 3
· 5 •Rate·lim1t1ng step
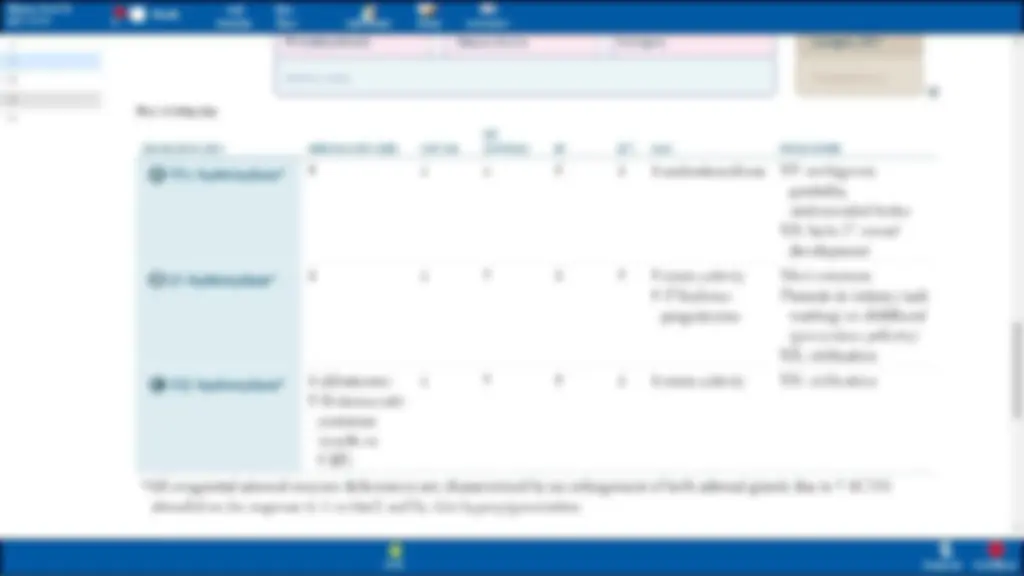
ENZYME DEFICIENCY
0 17 a-hydroxylasea
0 21 -hydroxylasea
~ 11 ~-hydroxylasea
X
MINERALOCORTICOIDS
t
l aldosterone
t 11-deoxycorti-
costerone (resu lts in
t BP)
CORTISOL
l
SEX
HORMONES BP^ [K•]
l t l
t t
t t
LABS
l androstenedione
t ren in ac tivity
t 17-hrdroxy-
progesterone
l renin ac ti vity
PRESENTATION
XY:ambiguous genitalia, undescended testes XX: lacks 2° sexual de\ elopment
Most common Presents in infancy (salt wasting) or c hi ldhood (precocious puberty) XX: vir ilization
XX: viri lization
:'All congeni ta l adrenal enzyme deficiencies are characterized^ by^ an enlargement of both adrenal glands due^ to^ t^ ACTH
stimulati on ( in response to l co rti sol) and by skin hyperpigmentation.
8 s^^8 Lode. Suspe-nd^ E^ nd^ Bloc:k
Item: 3 of S - , • Mark - "'I^ ~^ ··^ ~
QIO: 3020 ~^ P~v•ous^ N@xt^ Lab^ l lues^ Notes^ Calculator
1 2
· 3
· 5
An 8-day-old premat ure neonate is brought to t he pediat ri cian by his mother, who notesthathe^ cr^ ied all through the night. She al^ so^ says^ ~~AI thathe appears^ "floppy"^ lately and moves^ ve^ ry l^ ittle^.^ On^ physical examination,^ the^ newborn's skin appears yellow. His sclerae are also yellow. Testingofhis reflexes reveals decreased responses. The baby is subsequentlyadmitted t o^ the^ hospital.
Low levelsofwhichofthe following proteins worsen this pathology?
: A. Albumin
B. Ceruloplasmin
C. Ferritin
- Hemoglobin
E. Intrinsic factor
8 s^^8 Lode. Suspe-nd^ E^ nd^ Bloc:k
Item : 3 of S ~ , • Mark <::J [:::> "" I ~ · ~'j
QID: 3020 J.. Previous Next LAb faiUI~S Notes Calculator
1 2 3
T he co rr ect a n swe r is A. 50°/o chos e t h is.
Jaundice is a condit ion in which t he pat ient's sclerae and skin appear yellow as a resu lt of hyperbil iru bi nem ia. The pat ient in th is vi gnett e also has developed kernicterus, or excess unconj uga te d bilirubin damag ing the central ne rvous system (CNS), whi ch is characterized by neurologic defici ts incl uding hypot onia, lethargy, and poor ref lexes. Albumin bi nds unconj ugated biliru bi n in t he blood, and t he albumin-bilirubin complex is unable to pass t hrough the bloo d- brain barrier, pr event ing bi lirubin f rom aff ect ing the CNS. Lower levels of album in would result in less com pl exing of the uncon juga t ed bilirub in, increasing t he ri sk of kerni cter u s. Premat ure neonat es may be at increased risk of low album in level s, especially in the fi rs t few days of life. There are many causes of hyperbilirubinemia. Decreased hepat ic enz yme act ivi ty in the newborn, or even increased reabso rpt ion of bi lirubin from the gut (the "enterohepat ic circu lat ion" ), also ca n produce j aundi ce in the ne wborn. Jaundi ce and kernicterus also may occur in syndromes characte ri zed by a def iciency of t he hepat ic enz yme uri dine diphosphate-glucurony l t ra nsfe rase, which conj ugates bilirubin. T he result ing inabili ty t o co n juga t e bi lirubin leads to less excretion t hro ugh such vehicles as urine, and an increase in ser um bilirubin levels. A th ird ca use of hyperbilirubinem ia is increased hemolysis. There are many causes of increased hemolysis in a newborn, nota bl y heredi tary RB C defects such as spherocytosi s, infect ion, and maternal -fetal bl ood t ype incom pat ibilit y. The fi rs t -line t rea tment for hyperbiliru bi n em ia in t he neonate is phot otherapy; t reatment fo r ref ractory cases includes exchange t ransfusion. Photot he r apy is the use of light t o break down un conj ugat ed biliru bi n t o small er, water -soluble p ro ducts so they may be excret ed. Bilirubin Kernicterus Exchange transfusion Central nervous system Hyperbilirubinemia Hemolysis Hypotonia Light therapy Jaundice Blood-brain barrier Human serum albumin Albumin Enzyme Blood plasma Blood type Infant Urine Liver Sclera Neurology Red blood cell Nervous system Spherocytosis Blood transfusion Gastrointestinal tract Hypoalbuminemia
B is not co rr ect. 17 % c ho se thi s.
Ce ruloplasmin is a plasma protein t hat serves as the maj or storage protein for copper. A deficiency of ce rulo pl asmin may result in Wi lson disease, an autosomal recessive disease. Patients wi th Wi lson disease exhibit ne uropsychiat ric symptoms caused by deposit ion of co pper in t he basal gangl ia. Addit ionall y, copper may deposit aro und t he iri s, fo rming Kayser-Fleischer rings. Also, copper deposit ion in the liver leads t o liver fa ilure. Long- term management of Wilson disease includes copper chelat ion t herapy wi th D- penicill am ine and event ual liver t ra nsplantat ion. Ceruloplasmin Chelation therapy Basal ganglia Wilson's disease Liver transplantation Autosomal recessive Penicillamine Protein Chelation Dominance (genetics) Liver Blood plasma Autosome Blood proteins Liver failure Organ transplantation Copper Iris (anatomy) Neuropsychiatry
C is not co rr ec t. 11 % chos e thi s.
Ferr it in is t he main int racellul ar iro n- binding p rot ein. Low levels of f erri t in are indi ca t ive of an iron def iciency, which can be t rea te d wit h iron supplemen tat ion. During anemia of ch ronic disease, fe rr it in levels may act ually be elevated because of i ts role as an acu te - phase reactant and because of increased int race llular hoarding of iron. Ferrit in levels may also be elevated during iron overload disorders su ch as hemochromat osi s. These disorders are t reat ed wi th iron chelators. Anemia of chronic disease Ferritin Acute-phase protein Iron overload Anemia Protein Iron deficiency Chronic condition Chelation Iron
8 s 0 Lock S uspend End Block
Item: 3 of 5 - , • Mark -<] 1:> ""'I ~· 1!';:'
QIO: 3020 ~ Prev 1 o u s Next Labf a lues Notes Calculator 1 2 3
· 5
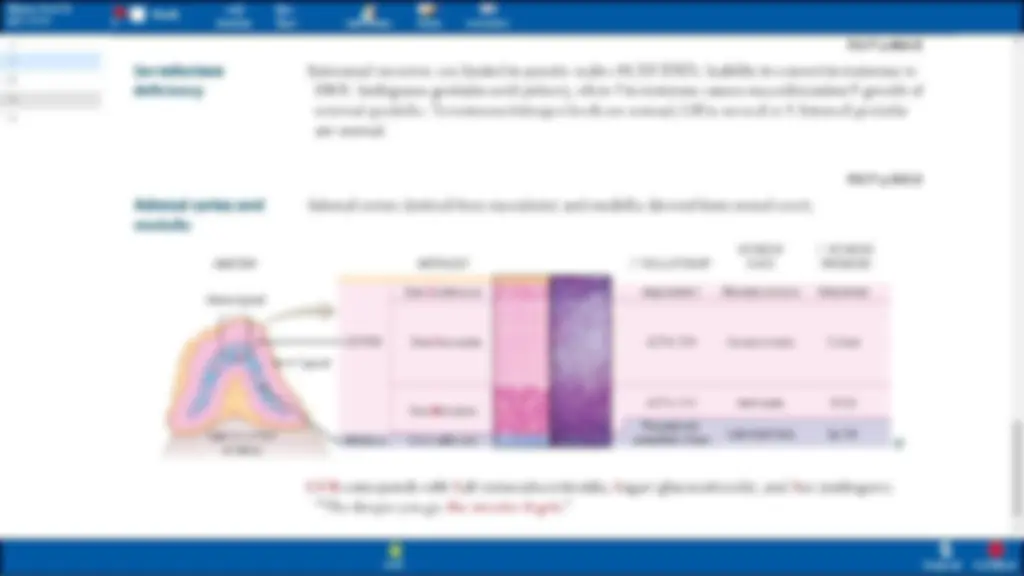
Jaundice
Unconj ug at ed
(indirec t)
hyperbilirubinemia
Conjugated (direc t)
hyperbilirubinemia
Mi xe d (direc t
and indirec t)
hyperbilirubinemia
Abnormal yellowing of the s kin and/or sclera duetobilirubin deposition. Hyperbilirubinemia 2° to t production or ! di sposition (impaired hepatic uptak e, conjugation, excretion).
FA17 p 376.
HOT Liver- common causes of increa se d le,els of bilirubin: Hemolysis Obstruction Tumor J.i,cr disease
He mol ytic, ph ysio logi c (newborns), Cr igler-Najjar, Gilbert syndrome.
Biliary tract obstruction: g<1llsto ncs, c ho langiocarcinoma, pancreati c orliver cancer,liver Aukc. Bili ary tract dis ease:
- 1° sclerosin g cholang itis
- 1° biliary cholangitis Excretion defect: Dubin-John so n sy ndrom e, Rotor sy ndrome.
Hepatitis, cirrh osis.
(^8) s ~
L.odt (^) Su~pl'nd End Block
Item: 3 of S - , • Mark - "'I^ ~^ ··^ ~
QIO: 3020 ~^ P~v•ous^ N@xt^ Lab^ l lues^ Notes^ Calculator
1 2 3
· 5
Hereditary hyperb i lirubinemias
0 Gilbertsyndro me
E) Crig ler-Najjar sy ndr ome, t ype^ I
E) Dubin-Johnson syndrom e
All autosomal recessive.
Mildly l UDP-glucuronosyltransferase conjugati on a nd impaired bilirubin uptake. Asymptomatic or mild jaundice usually^ with stress,illness, or fasting. t unconjuga^ ted bil irubin without overt hemolrsis. Biliru bin ' t'' ith fasting a nd s tress.
Abse nt UDP-glucuronosyltransfcrase. Presents early inlife;pati^ ents die within^ a^ fc" years. Findings: jaundice, kernicte ru s (bilirubin depos ition in bra in), t un co njugated bilirubi n. Treatment: plasmapheres^ is and^ phototherapy.
Conjugated hype rb ilir ubin e mi a clue to defecti ve liver excretion. Grossly black liver. Benign.
FA17 p 377.
Relati,-eJy common, benig n condition.
TypeIIis less^ se,·ere^ and res^ po^ nd^ s^ to phenoba rbit al, whi ch^ t^ Ji,·er^ enzymesynthesis.
e Rotor syndrome is similar, but milderin presentation without blackli ver.Due to impaired hepatic uptake and excreti^ on.
HEPAT SINUSOID
Circutatmg bilirubin --- Hemoglobin Kuptfer ceO plla~
j 1 ll I
8 s^^8 Lode. Suspe-nd^ E^ nd^ Bloc:k
Item: 4 of S - , • Mark - "'I^ ~^ ··^ ~
QIO: 2346 ~^ P~v•ous^ N@xt^ Lab^ l lues^ Notes^ Calculato r
1 2 3
· 5
Two weeksafterinitiationof diu retic therapy to control essential hypertension, a^ 51-year-old^ man presents t o his physicianfora check-up.^ ~~AI Physi^ ca^ l^ examination^ revea ls^ a^ blood^ pressureof^ 130/85^ mm^ Hg. Laboratory tests show a^ blood^ pH of^7 .48, an^ arterial^ partial^ pressureof carbon dioxideof 50 mmHg, and a bicarbonat e^ level^ of41 mEq/L.
Whichofthe following causes is most consistentwiththis^ clinical^ situation?
A. Acetazolamide-induced metabolic alkalosis
B. Acetazolamide-induced respiratory alkalosis
C. Hydrochlorothiazide-induced metabolic^ alkalosis
0. Hydrochlorothiazide-induced respiratory^ alkalosis
:
8 s^^8 Lode. S uspe-nd^ E^ nd^ Bloc:^ k
Item: 4 of S ~ , • Mark <::J [:::> "" I ~ · ~'j QID: 2346 J.. Previous Next LAb faiUI~S Notes Calculator 1 2 3 4
. 5
The c orrect answer is C. 72 °/o c ho s e this.
Hydrochlorot hiazide and furosemide cause met abolic alkalosi s. Note t hat t he elevated pH ind icates an alkalosis, and t he elevated bi ca rbonate and ca rbon dioxide indicate a met abolic alkalosis wi th part ial respirat ory compensation. Bo t h th iazides and loop diuret ics inhi bit sodium upt ake, and t hus increase delivery of sodium distally to the late distal tu bu le and collecting duct. An increased amoun t of sodium is taken int o t hese dist al cells f rom t he lu minal surface and exchanged for potassium and protons t o maint ain elect roneut rality. This creat es a condit ion of hypokalemia (too litt le potassium in the blood), kaliuresis (uri nat ion of excess potassi um), and excess uri nary acid secret ion. This loss of acid promotes me tabolic alkalosi s. In addit ion, hypokal em ia induces t he movement of pot assi um from i ts vast st orehouse wi th in t issues to t he ex tracell ular com partment in exchange f or hydrogen ions. This movement of pot assiu m f rom t issues in to blood and protons from the blood i nto t issues f u rt he r promotes me tabolic alkalosi s. In short, serum pot assi um levels t ends to change in t he same direction as t hat of serum protons. Hydrochlorothiazide Furosemide Metabolic alkalosis Hypokalemia Distal convoluted tubule Carbon dioxide PH Thiazide Collecting duct system Alkalosis Loop diuretic Diuretic Bicarbonate Sodium Potassium Respiratory compensation Blood plasma Lumen (anato,.,) Nephron Kaliuresis Metabolism Hydrogen Proton
A is not correct. 22% chos e this.
Acet azolamide impai rs reuptake of bica rbo nat e and secr et ion of acid in t he proximal tub ule. The loss of bica rbo nat e in t he urine leads to metabolic acidosis. Acetazolamide Metabolic acidosis Proximal convoluted tubule Acidosis Bicarbonate Urine Nephron Metabolism
B is not correct. 3% chose this.
This pat ient 's labor atory values are consist ent wit h me tabolic alkalosis wi th respi r atory com pensat ion. Acetazol am ide fu nct ions by im pairi ng reuptake of bi carbo nate and secret ing acid wit hin t he proxi ma l tu bule, t hus you would expect to see me tabolic acidosis wit h t he use of th is agent. Acetazolamide Metabolic alkalosis Metabolic acidosis Proximal convoluted tubule Respiratory compensation Acidosis Bicarbonate Alkalosis Metabolism Nephron
D is not correct. 3°/o chose this.
This pat ient 's labor atory values are consist ent wit h me tabolic alkalosis wi th respi r atory com pensat ion. Hydrochlor ot hiazide causes a met abolic, not a respiratory, alka losis. Hydrochlorothiazide Metabolic alkalosis Respiratory compensation Alkalosis Metabolism
Bottom Line:
Hydrochlorot hiazide and furosemide are diur et i cs capable of inducing metabolic alkalosis. Laborat ory values consistent wit h meta bolic alkalosis in cl ude elevated pH, elevat ed part ial a rt erial ca rbon dioxide pressure, and elevat ed bi ca rbo nat e level.
8 s 0 Lock Suspend End Block
Item: 4 of S - , • Mark - "'I^ ~^ ··^ ~
QIO: 2346 ~^ P~v•ous^ N@xt^ Lab^ l lues^ Notes^ Calculator
1 2 3 4
· 5
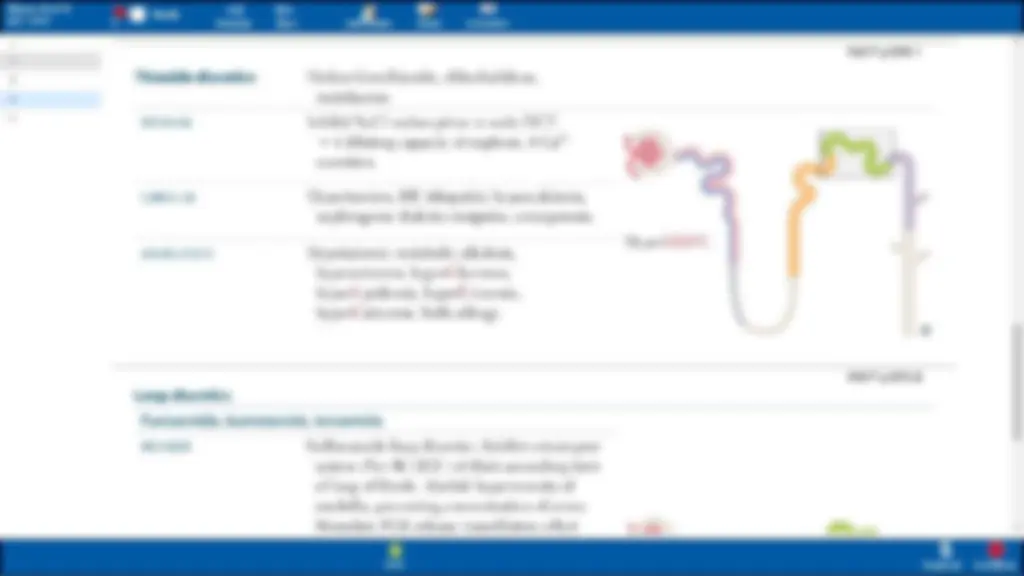
Thiazide diuretic s
MECHANISM
CLINICAL USE
ADVERSE EFFECTS
Loop diuretics
Hydrochlorothiazide, chlorthal idone, me tohlZone.
Inhibit aCI reabsorption in early DCT ... l diluting capacity of nephron. l Ca 2 + excretion.
llrpertension, HF, idiopathichypercalc iuri a, nephrogenic diabetes insipidus,osteoporosis.
Hypokalemic metabolic a lkal osis, hypo natremia, hyperGlycemia, h) perLipidemia, hype rUricemia, hype rCalcemia.^ Su^ lfa^ allergy.
Furosemide, bumetanide, torsemide
MECHANISM Sulfonamide loop diuretics. Inhibit cotranspo rl sys tem (N a•fK+f2C l-) of thick ascending limb ofloop of Henl e. Abol ish hypertonicity of medu lla , pre,·e nting conce nt rat ion of urine. Stimulate PGE release (vasodilatorv effect
FA17p576.
HyperCLUC.
FA17 p 575.
8 s^8 Lode. Suspe-nd^ E^ nd^ Bloc:k
Item: 4 of S - , • Mark - "'I^ ~^ ··^ ~
QIO: 2346 ~^ P~v•ous^ N@xt^ Lab^ l lues^ Notes^ Calculato r
1 2 3 4
· 5
loopdiuretics
Furosemide, bumetanide, torsemide
MECHANISM^ Sulfonamide^ lo^ op diuretics. Inhibit co^ transport
CLINICAl USE
ADVERSE EFFECTS
Ethacrynic acid
MECHANISM
CLINICAL USE
ADVERSE EFFECTS
system (Na+JK+f2CJ-) of thick^ asce^ nding^ limb of loo p of Henl e.Abolish hypertonicity of medulla, pre,·enting concentration of urine. St imulate PG^ E^ release^ (vaso^ dil^ atory^ effect on afferent arteriole); inhibited by NS IDs. f Ca 2 + excretion. Loo^ ps Lose^ Ca2^ +.
Ed ematous states (1-1 F', ci rrh osis, nephrotic syndrome, pulmonary ede ma), hype rt ension, hypercalcemia.
Ototoxicity,Ilypokalemia, I lypomag n ese mi a, Dehydration, Allergy^ (s^ ulfa^ ), metabolic Alkalosis,Nephritis (interstitial),Go^ ut.
lon sulfonam ide inhibitor of cotransport system (Na +JK+f2C^ J-) of^ I^ hick ascending limb^ of loo^ p of Henl e.
Diures is in patients allergic to sulfa dru gs.
Sim ilar to furo se mid e, bu t more ototox^ ic.
FA17 p 575.3 •
Ollll^ DAANG!
Loop ea rrin gs hurt yo ur ears.
8 s^8 Lode. S u^ spe-nd^ E^ nd^ Bloc:k