Download USMLE Renal Pathology Essentials 2025/2026: Diseases of the Kidney and Urinary Tract and more Exams Medicine in PDF only on Docsity!
Item: 1 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 4749 ..L a r Pre v ious Next^ Labfli!llues^ Notes^ Calcula t o r
· 8
. 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
A 67-year-old man admittedfor postoperative recovery is foundto^ be^ oliguric.^ Laboratory^ studies^ show^ a^ blood^ urea^ nitrogen^ level^ of^200
mg/dland a serum creatinine level of 6 mg/dl. Urinalysis shows:
Specificgravity: 1.
Urine osmolality: 670 mOsm/kg
Sodium: 14 mEq/L
BUN/Creatinine ratio: 56
Fractional excretionofNa:^ 0.54%
Protein: negative
Casts: negative
Whichof the following isthe most likely causeof^ this^ patient's^ oliguria?
A. Acute interstitial nephritis
B. Acute tubular necrosis
C. Bladder calculus
D. Heart failure
E. Nephrotic syndrome
a s^8
&
Item: 1of24 ~. ,. M k <:] t> al ~· ~
QIO: 4749 .l. ar Previous Next Lab 'lifllues Notes Calculator
· 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
The co rr ect a n swe r is 0. 4 80/o c h ose t hi s. This pati e nt's labo rato ry tests confirm the classic criteria for d ia gnos ing prer ena l azo temia. Prer ena l azo temia is caused by a r educt ion of the g lome rular filtrati on rate (GFR} provo ked by an insult to the vascular supply to the ki dney. Causes of prer ena l azo temia inclu de hea rt failure, sepsis, and r ena l artery stenosis. The r educt ion in GFR increases the accumulation of b ot h blood urea nitrogen (BUN} and creatinine (Cr} in the bl ood, but because the B UN concentration in blood is dete rmin ed by b oth g lome rular filtrati on and reabso rpti on (in contrast to C r, which is limited to filtrati on and not reabso rb ed} , the B UN leve l rises out of propo rti on to the Cr leve L This therefore elevates the B UN :Cr rati o. I n addition, this pati ent 's fractional exc r et ion of sodium ( FeNa) is less than 1%, ind icativ e of a prer ena l cause. If the FeNa is g r eate r than 2%, an intrinsic r ena l o ri g in, such as acute tubular necrosis, is the cause. Of the causes listed here, heart failure is the most likely o pti on for a prer ena l cause. Renal artery stenosis Blood urea nitrogen Azotemia Renal function Acute tubular necrosis Urea Creatinine Sepsis Fractional sodium excretion Kidney Renal artery Glomerulus Sodium Glomerulus (kidney) Stenosis Necrosis Blood vessel Nitrogen Heart failure Excretion
A is n ot co rr ect. 1 50/o c h ose t his. Acute inte rstitial nephritis (A I N} is an intrarena l cause of azo temia caused by inflammati on due to a number of factors, includ ing toxins and d ru gs. AI N usually manifests with eosino philic casts in the urine and with findings similar to acute tubular necrosis (A T N}, includ ing an elevated fractional exc r et ion of sodium. Interstitial nephritis Acute tubular necrosis Nephritis Azotemia Fractional sodium excretion Urine Interstitial fluid Sodium Necrosis Inflammation Excretion
B is n ot co rr ect. 200/o c h ose t his. Acute tubular necrosis (A T N} can mimic prer ena l azo temia in many ways, although it is essent ially an intrarena l azo temia. However, the maj or d istin gu ishing features that make this pati ent unlikely to have ATN are the absence of casts in the urine, the high urine - specific g ravity (A TN usually causes nonoliguric azo temia), and the very high B UN :Cr rati o. I n addition, in ATN the fractional exc r et ion of sodium is usually >2%, which is not the case in this pati ent. Acute tubular necrosis Azotemia Fractional sodium excretion Necrosis Sodium Urine Excretion
C is n ot co rr ect. 130/o c h ose t his. Bla dde r calculi are a maj or cause of p ost r ena l azo temia, which is d istin gu ished from prer ena l azo temia by the re lativ ely normal B UN :Cr rati o and, more imp o rtantly, the lack of highly concentrated urine. This pati ent 's B UN :Cr rati o, urine specific g ravity, and fractional exc r et ion of sodium suggest the presence of prer ena l azo temia. Specific gravity Azotemia Fractional sodium excretion Urine Urinary bladder Sodium Excretion
6 s 0
Item: 1 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 4749 ..L a r Pre v ious Next^ Labfli!llues^ Notes^ Calcula t o r
· 8
. 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
&
Acutekidneyinjury
(acute renal failure)
Preren al azote^ mi^ a
Intr insic ren al failure
Postrenal azot emia
FA17 p 571.
Acute kidn^ ey^ injuryis^ defined^ as^ an^ abruptdeclineinrenal^ fun^ ctionasmeasured^ by^ t^ creatinine a nd t BU! or by oliguria/anuria.
Due to l RBF (eg, hypotemion) -^ l^ CFR.^ la•/^1110 and BUt^ retained^ by^ kidney^ inan atte^ mpt^ to consen e vo lume - t BU '/creatinine ratio (BUNisrea bso rbed, creatinine is not) and^ l^ F'E'Ia· C enerallr due to ac ute tubular necros is or ische mi a/toxins;lesscommonly due to^ ac^ ut^ e glomer ul onephritis (eg,RPCN,^ hcmol)^ Lieuremic^ S)^ ndrome) oracute i^ nterstitial nephritis. In ATN, patchy necrosis - de brisobstructing tubule and Auid backAow acrossnec^ roti^ c tubule
- l C FR. Urin e hasepithelial/granular^ c~^1 sts.^ BU!':^ reab^ sorptionis impa^ ired -^ l^ BUI':/crcatininc ratio and t FENa· Due to outflowobstruction (ston es, BPI I, n eoplasia, co nge nital anomalies).^ D^ e,·elo^ ps^ only^ w^ ith bil ateral obstruction.
Urine osmolality
(mOsm/kg)
Urine Na + (mEq/l)
FENa
Serum BUN / Cr
Prerenal
> 500
<2 0 < I%
> 20
Intrinsic renal
<^350
> 40
>2%
< 15
Postrenal
< 350
> 40 < 1 % (mild ) > 2% (se ,·ere) Varies
FA17 o 562.
a s^8
&
Item: 1 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 4749 ..L a r Pre v ious Next^ Labfli!llues^ Notes^ Calcula t o r
· 8
. 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
Casts in urine
'
RBC casts
WBC casts Fatty casts ("oval fat bodies")
Granular (" muddy brown ") casts
Waxy casts I!]
Hyaline cast s 0
FA17 p 562.
Presence ofcasts indicates that hematuria/pyuria isofglomerular or renal^ tubular^ origin. Bladder cancer, kidney stones -^ hematuria,^ no^ casls. Acute cystitis - pyuria, no casts. Glomerulonephritis, malignant hypertension.
Tubulointerstitial inAamma tion, acute pyelonephritis, transplant rejection.
' ephro tic syndrome. Associated with^ ··^ i^ laltese^ cross"^ sign.
Acute tubular necrosis.
End-stage renal disease/ch ronic renal failure. 1'\onspecific, can be a norma l finding, often seen in co ncent rated urine samples.
a s^8
&
Item: 2 of 24 ~. I • M k <:] t> al ~· ~
QIO: 4162 .l. ar Previous Next lab 'lifllues Notes Calculator
· 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
The co rr ect a n swe r is 0. 4 50/o c h ose t hi s. I n young, he althy w ome n with su dde n -o nset hyp e rtensio n, it is im po rtant t o consi de r inhere nt structural de fe cts of th e renal arte ry wall that m ay impair pe rfusi on of one or bo th kid ne ys. These de fe cts are t e rm ed fibr o muscular d ysplasias. De creased pe rfusi on lead s t o stimulati on of th e renin -an g iot ensin -al do sterone ax is, re sultin g in syste mic vasoco nstricti on an d vo lum e ex pansi on. If th e cond iti on is unilateral, ultras ound may de mo nstrate one atro phic kid ney an d if ad vanced, co ntralateral hyp e rtro phy of th e unaffe cted kid ney. Re nal arte ry stenosis of this typ e is be st tre ated with surge ry, which can th en he lp relieve th e second ary hyp e rtension. Renal artery stenosis Vasoconstriction Secondary hypertension Renal artery Ultrasound Stenosis Hypertension Medical ultrasound Kidney Hypertrophy Perfusion Anatomical terms of location Contralateral Atrophy
A is n ot co rr ect. 130/o c h ose t his. A thro mb oe mb olus in th e renal arte ry may cause new -o nset hyp e rtensio n; how eve r, it is unlik ely t o be th e cause in this young, o th e rwis e he althy pati e nt. T hro mb oe mb oli t o th e renal arte ry o ften o ri g inate in th e le ft he art, e ith er after my o card ial infarcti on or re sultin g fr om bacterial v ege tati ons seen in bacterial en do card itis. An acute e mb olus w o ul d likely cause a sp e ctrum of o th er sympto ms an d co ul d re sult in infarcti on of th e affe cted kid ney. Myocardial infarction Embolism Embolus Endocarditis Hypertension Renal artery Kidney Infarction Heart
B is n ot co rr ect. 180/o c h ose t hi s. A th erosclerosis of th e renal arte ry is a more co mm on cause of su dde n -o nset hyp e rtension but w o ul d more likely be susp e cted in ind ivid uals over 5 0 ye ars old or with pred isposin g cond iti ons (eg, d iabet e s). S imilarly t o fibr o muscular d ysplasia, de creased pe rfusi on of one or bo th kid ne ys lead s t o stimulati on of th e renin -an g iot ensin -al do sterone ax is, re sultin g in syste mic vasoco nstricti on an d vo lum e ex pansi on. Re nal arte ry stenosis of this typ e is be st tre ated with co nv e nti onal balloon an g io plasty. Fibromuscular dysplasia Renal artery stenosis Atherosclerosis Vasoconstriction Renal artery Angioplasty Stenosis Hypertension Diabetes mellitus Perfusion Kidney
C is n ot co rr ect. 1 60/o c h ose t his. Conn syn d rome is caused by an al do steron e- se cre tin g a de no ma of th e ad renal co rtex an d is a fo rm of hyp eral do stero nism. It may re sult in new - onset hyp e rtension an d is o ften asso ciated with o th er syste mic sympto ms (alkal osis an d hyp okale mia). If th e pati e nt had an al do steron e- se cre tin g tum o r, sh e w o ul d be ex pe cted t o hav e low plasma renin. Hypokalemia Primary aldosteronism Adrenal cortex Hyperaldosteronism Hypertension Renin Blood plasma Alkalosis Adenoma Neoplasm Adrenal gland
E is n ot co rr ect. 80fo c h ose t his.
~ · '^.^ r^ oo^ ' " '^0
6 s 0
Item: 2 of 24 ~. I • M k <:] t> al ~· ~
QIO: 4162 .l. ar Previous Next lab 'lifllues Notes Calculator
1 2
· 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
B is n ot co rr ect. 180/o c h ose t hi s. At herosclerosis of the r ena l artery is a mo re common cause of sudden -o nset hyp e rtens ion but would mo re likely be suspected in ind ivi dua ls ove r 50 years old or with pred isposing conditions (eg, d iab etes). S im ilarly to fibromuscular dys plasia, dec reased pe rfusi on of one or b oth ki dneys leads to stimulation of the ren in - angiotensin - aldosterone axis, resu lting in systemic vasoconstriction and volume ex pansi on. Rena l artery stenosis of this type is b est treated with conventional balloon angioplasty. Fibromuscular dysplasia Renal artery stenosis Atherosclerosis Vasoconstriction Renal artery Angioplasty Stenosis Hypertension Diabetes mellitus Perfusion Kidney
C is n ot co rr ect. 1 60/o c h ose t his. Conn syndrome is caused by an aldosterone - secreting adenoma of the adrenal cortex and is a form of hyperaldosteronism. It may resu lt in new - onset hypertension and is often associated with othe r systemic symptoms (alkalosis and hypokalemia). If the pati ent had an aldosterone - secreting tumor, she would be ex p ected to have low plasma ren in. Hypokalemia Primary aldosteronism Adrenal cortex Hyperaldosteronism Hypertension Renin Blood plasma Alkalosis Adenoma Neoplasm Adrenal gland E is n ot co rr ect. 80/o c h ose t his. Pheoch r omocytoma is a catecholamine - secreting tumor of the adrenal medulla. I ncreases in plasma epin e phrin e and norepinephrine cause relapsing and r em ittin g symptoms such as hypertension, d iaphoresis, headaches, and heart palpitati ons. Howeve r, plasma ren in leve ls would not be increased in the setting of ph eoch r omocytoma. Approximately 50% of pati ents have hypertension at baseline, not j ust paroxysm ally, an inter est ing physical exam finding in these pati ents is o rth ostat ic hypotension. Because the tumor still secretes low leve ls of catecholamines at baseline the vasculature in these pati ent 's is already maximally constricted, upon standing they are unable to constrict their vessels further, resu lting in o rth ostat ic hypotension. When systemic vasculature is maximally constricted, ren in will not be released and is low in these pati ents. Pheochromocytoma Orthostatic hypotension Epinephrine Adrenal medulla Norepinephrine Perspiration Renin Hypotension Hypertension Catecholamine Blood plasma Circulatory system Palpitations Vascular resistance Neoplasm Medulla oblongata Adrenal gland Physical examination
Botto m Line : Sudden-onset hypertension can be associated with r ena l artery stenosis, in which fibromuscular changes to the r ena l artery impair pe rfusi on of the ki dney. Renal artery stenosis Renal artery Hypertension Stenosis Perfusion Kidney
6 s 0
Item: 3 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 18 0 6 ..L a r Pre v ious Next^ Lab^ fli!ltues^ Notes^ Calcula t o r
. 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
A 50 - year -old manisadmitted to the hospital. His drugregimen^ includes^ furosemide,^ a^ loop^ diureticthatacts on the^ sodium-potassium-
chloride symporterin theascending limb ofthe^ loop^ of^ Henle.^ The^ patient's^ treatingphysicianmustdecide^ which^ medications^ to^ continue
during the patient's hospital stay.
The presenceofwhich ofthe^ following^ conditions^ in the^ patient^ would^ promptthediscontinuationoffurosemide?
A. Exacerbationofcongestiveheart^ failure
B. Hyperkalemia
C. Hypocalcemia
D. Nephrotic syndrome
E. Worsening hypertension
a s^8
&
Item:3of24 ~. ,. M k <:] t> al ~· ~
QIO: 1806 .l. ar Previous Next lab 'lifllues Notes Calculator
1 2
. 4
· 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
The correct answer is C. 680/o chose this. Furosemide is a loop d iuret ic that inhibits the sodium - potassium - chloride co - transporter, and at max i ma l dosage , can exc r ete about 25% of filtered sodium. The reabso rpti on of calcium in the loop of Hen le is primarily passive, being d riv en by the g rad ient created by sodium and chloride transport. With furosemide, this g rad ient is dest r oyed. Because it promotes the exc r et ion of calcium, furosemide is used to treat hyp e rcalcem ia, but it is contraindicated in a hyp oca lcem ic state. loop diuretic Furosemide Diuretic Hypercalcaemia loop of Henle Calcium Sodium Hypocalcaemia Reabsorption
A is not correct. ]Ofo chose this. A pati ent with an exace rbati on of congestive heart failure (CH F} is a good candidate for furosemide. I n decom p ensated CH F, pati ents are volume ove rl oaded, and as a resu lt, may hav e pulm ona ry edema and ex pe ri ence d ifficulty breat hing. Furosemide will encou ra ge d iuresis and he lp the b ody mobili ze the excess flui d, clearin g the lun gs and helping that pati ent breat he b ette r. Furosemide Pulmonary edema Heart failure Congestive heart failure Diuretic Edema Forced diuresis Polyuria lung
B is not correct. 11 Ofo chose this. Hy pe rkal em ia is a serious condition because of the poss ibility of deve lopin g an arrhythmia. Patients should be treated when ECG changes are present (spiking of the T wave) or if serum potass ium r eac hes > 7.0 m Eq/ L. I nitial treatment may inclu de calcium, which will antagoni ze the membrane actions of hyp e rkal em ia to he lp prevent arrhythmia, along with insulin and g lucose, which he lp to pull the potass ium from outs ide to insi de the ceiL The pati ent also may receive sodium po lystyrene ( K ayexalate), a gast ro intest inal syrup that works more slowly by ri dd ing the b ody of potass ium through the stooL Loop d iuret ics such as furosemide actually may be used to he lp with hyp e rkal em ia as well, as they increase exc r et ion of potass ium. Furosemide Hyperkalemia Cardiac arrhythmia Potassium Diuretic Electrocardiography T wave Sodium Polystyrene sulfonate Insulin Polystyrene loop diuretic Glucose Calcium Blood plasma Serum (blood) Equivalent (chemistry) Human gastrointestinal tract Gastrointestinal tract 0 is not correct. 90fo chose this. Nephrotic syndrome is characteri zed by massive prote inuria, hyp oa lbumin em ia (because of loss of albumin in urine), edema, and hyp erch oleste rolem ia. Whereas the treatment of nephrotic syndrome is targeted at the underlying d isease (which can be qu ite varied}, d iuret ics like furosemide^ also^ are^ used^ to^ treat^ the^ edema^ associated^ with^ this^ syndrome^. Furosemide Nephrotic syndrome Hypoalbuminemia Proteinuria Human serum albumin Hypercholesterolemia Edema Albumin Urine Diuretic
E is not correct. 50fo chose this.
6 s 0
Item: 3 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 18 0 6 ..L a r Pre v ious Next^ Lab^ fli!ltues^ Notes^ Calcula t o r
· 4
· 8
. 9
&
FA17 p 575.
loopdiuretics
Furosemide, bum etanide, torsemide
MECHANISM Sulfonamideloop diuretics.^ Inhibit^ cotransport
CliNICAl USE
ADVERSE EFFECTS
Ethacrynic acid
MECH ANISM
CLINICAL USE ADVERSE EFFECTS
system (Na+fK+f2CI-) of thid. ascending limb of loop ofllc nlc. boli sh hyperton icit} of medulla, preve nting concentration of urine. Stimulate^ PCE^ release ('asodilatory effect on afferent arteriole); inhibited b) NSAIDs. f Ca 2 + excretion. Loops Lose^ Ca^2 •^. Edematous states (HF, cirrh osis, nephrotic syn drome, pulmonar} edema),h)perlens ion , hypercalcem ia^. O totox ici ty, I lypokalemia, I Jypomagnesemia, Dehydration, Allergy (sulfa),metabolic Alkalosis, Nephritis (int^ ers^ titial), Gout.
~onsulfo namide inhibitor of co transport sys tem ( a•fK+f2CI -) of thick ascending limb of loop of ll enle.
Diuresisin pati ents allergic to s ulfa dru gs.
Similar to furosemide, but more ototo,ic.
Ollll D.\Al':C!
Loop earrin gs hurt rour ears.
a s^8
&
Item: 3 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 18 0 6 ..L a r Pre v ious Next^ Lab^ fli!ltues^ Notes^ Calcula t o r
. 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
CLINICAL USE
ADVERSE EFFECTS
( la+JK+fZCl-)^ of thi^ ck^ ascending limb^ of^ loop ofllcnle.
Diuresisinpatients allergicto^ sulfa^ dmgs.
Similar to^ furosemide, but more ototo,ic.^ Loop earrings hurt your^ ears.
FA17 p 576.
Diuretics: electrolyte changes
Urine NaCI^ t^ with^ all diuretics (strength varies based on^ potency^ of diuretic effect). Serum^ _^ aCl^ may^ decrease
Urine K•
Bloo d pH
Urin e Ca 2 +
asa result.
t especially^ with^ loop and^ thiazide^ diuretics. Serum K+^ may^ decrease^ as^ a result. l (acidem ia):carbonic anhydrase inhibitors: l IIC0 3 - reabsorption. K+ sparing: aldosterone blockade prevents K~ sec retion^ and^ II^ +secretion. Additiona^ lly,hyperkalemia leads^ to^ K+^ entering allcells^ (,·ia^ H+fK+ exchanger)^ in^ exchange^ for^ H^ ..^ exiting cells^. t (alkalemia):loop diuretics 2
' 4
· 8
. 9
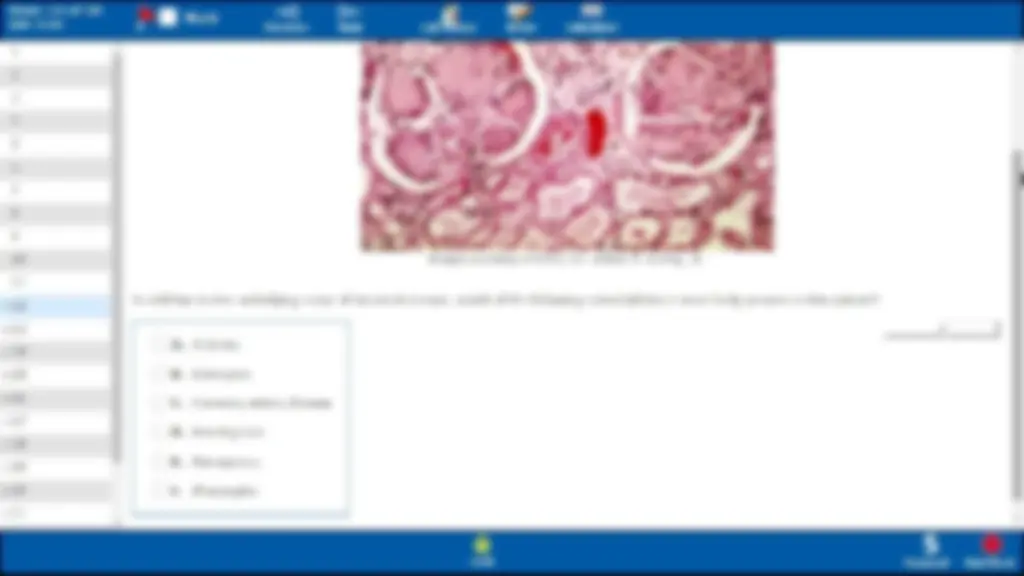
Whichofthe following risk factors hasthe strongestassociationwith this patient's disease?
A. A mutation inthe VHL gene on chromosome 3
B. A mutation^ of^ the^ WT1^ gene^ on^ chromosome^11
C. Historyof another primary tumor
D. History of heavy cigarette smoking
E. History of schistosomiasisinfection
a s^^8
Item:4of24 ~. ,. M k <:] t> al ~· ~
QIO: 4694 .l. ar Previous Next lab 'lifllues Notes Calculator
· 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
The correct answer is 0. 690/o chose t his. This pati ent has transitional cell carcinoma of the bla dde r, as ev idenced by his painl ess hematuria and absent signs of prostate cancer. Histology confirms the d ia gnos is with the presence of invasiv e transitional cells and prom in ent, atypical nuclei. Numerous factors increase the risk of deve lopin g transitional cell carcinoma, the most significant of which is an extens ive history of cigarette smoking. Ciga r ette smoking increases a pati ent 's risk by three - to sevenfold. Tr eatment of transitional cell carcinoma large ly de p ends on the stage of d isease, although these tumors have a tendency to recu r r ega rd less of d isease stage. Low-g ra de lesions may be treated with excision, whereas higher -g ra de lesions r equ ire a combination of excision and chemotherapy. Transitional cell carcinoma Hematuria Histology Prostate cancer Chemotherapy Urinary bladder Prostate Carcinoma Cancer Transitional epithelium Tobacco smoking Neoplasm Epithelium Cell nucleus Cigarette
A is no t correct. 10 0/o chose t his. A mutation in the VHL gene of chromosome 3, which causes von H ipp ei-Li ndau syndrome, is associated with a higher risk of r ena l cell carcinoma, rath er than transitional cell carcinoma of the bla dde r. Von Hippel-lindau syndrome Transitional cell carcinoma Renal cell carcinoma Gene Mutation Chromosome 3 (human) Urinary bladder Carcinoma VHl Chromosome Von Hippel-lindau disease Kidney
B is no t correct. 50fo chose t his. A mutation in the WT1 gene on chromosome 11 would place this pati ent at higher risk of Wilms ' tumor, a malignant neoplasm of r ena l mesenchymal cells. Wilms tumor is uncommon in adults. Wilms ' tumor WTl Neoplasm Gene Chromosome 11 (human) Mutation Chromosome Cancer Malignancy Mesenchyme Mesenchymal stem cell Kidney
C is no t correct. 50fo chose t his. T ransiti ona l cell carcinomas are primary tumors, rath er than metastases from othe r locat ions. T ransiti ona l cell carcinomas themselves often metastasi ze to othe r locat ions, especially the spinal column and othe r b ones. Metastasis Vertebral column Neoplasm Transitional cell carcinoma Primary tumor Carcinoma Epithelium
E is no t correct. 11 Ofo chose t his. Sch istosom iasis infect ion (eg, in a pati ent with travel to an endem ic area, includ ing the Midd le East) is a risk factor for the deve lo pm ent of squamous cell carcinoma; however, smoking is the most significant risk factor. Furthermore, a history of schistosomiasis in a pati ent who has never traveled outs ide of the United States would be unlikely.
6 s 0
Item: 4 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 4694 ..L a r Previous Next Lab^ fli!ltues^ Notes^ Calculat o r
· 8
. 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
Schistosomiasis Squamous-cell^ carcinoma^ Endemism^ Riskfactor^ Infection United^ States^ Squamous^ epithelial^ cell^ Middle East Carcinoma
Botto m line :
Transitional cell carcinoma^ oftenpresen^ ts^ with^ painless^ hematuriaand^ constitutional^ symptoms.^ Incid^ ence is influe^ nc^ edbyanumberofrisk
factors, i ncluding smoking,^ anilin e^ dye e^ xposur^ e, and^ cyclophosphamide^ use.
HematUI T a1 sitional^ eel^ carcinoma^ Cyclophosphamide^ AnilinecarcinomaAn^ 1ne^ dye^ Epithelurn^ Dye
I@ I ;J'.i 1;1 I•J fory ear: 20 17 ... FIRST AID FACTS
Transitional cell carcinoma
lost common tumor of urinary^ tra^ cl^ system (can occ ur in renal calyces, renal pelvis, ureters, and bladd^ er)^ fJ^ IE).^ Can be su^ gge^ sted by painlesshematuria (no casts). Assoc iated wit h problems inyour^ Pee^ SAC^ : Phe na ce tin , Smokin g, A ni line dyes, and Cycl o ph os phamide.
FA17 p 569.
a s^^8
&
Item: 5 of 24 ~ 1 • M k^ -<:J^ 1>-^ Jil^ ~·^ !:';-~
QIO: 4741 ..L a r Pre v ious Next^ Labfli!llues^ Notes^ Calcula t o r
. 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 2 0
- 21
&
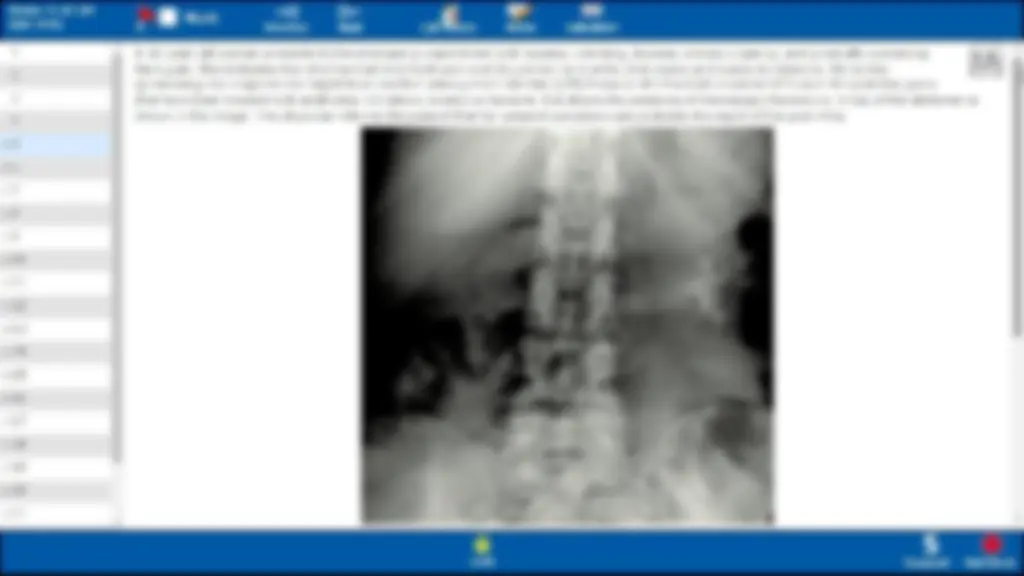
A 30 - year -old woman^ presents^ to^ theem erge^ ncydepartmentwithnausea,vomiting,dysuria,^ urina•·y^ urge^ ncy,an d grad^ ually^ worsening
flank pain. She indicatesthatshe hashadmild flank pain and discomfortformonthsthatwaxes^ and^ wan^ es inintensity.^ On^ further
questioning she suspects shemighthave anoth erurinary tractinfection^ (UTI)^ because she^ has^ hadrecurrent^ UTis^ over^ the^ pastfew^ years
thathave been treated withantibiotics. Urinalysis revealsno^ bacteria,butshowsthepresenceofmicroscopic^ hematuria.^ X-rayoftheabdomen^ is
shown in the image. Thephysicianinforms^ the^ patientthather^ present^ symptoms^ are^ probably^ the^ resultofherpast^ UTis.
a s^8