



EXODONCIA III
ACCIDENTS AND COMPLICATIONS
Dr. José María Aguado
Dra. María Luisa Martínez
Dr. Alberto Herranz










































Prepara tus exámenes y mejora tus resultados gracias a la gran cantidad de recursos disponibles en Docsity

Gana puntos ayudando a otros estudiantes o consíguelos activando un Plan Premium

Prepara tus exámenes
Prepara tus exámenes y mejora tus resultados gracias a la gran cantidad de recursos disponibles en Docsity
Prepara tus exámenes con los documentos que comparten otros estudiantes como tú en Docsity
Encuentra los documentos específicos para los exámenes de tu universidad
Estudia con lecciones y exámenes resueltos basados en los programas académicos de las mejores universidades
Responde a preguntas de exámenes reales y pon a prueba tu preparación
Consigue puntos base para descargar
Gana puntos ayudando a otros estudiantes o consíguelos activando un Plan Premium
Comunidad
Pide ayuda a la comunidad y resuelve tus dudas de estudio
Ebooks gratuitos
Descarga nuestras guías gratuitas sobre técnicas de estudio, métodos para controlar la ansiedad y consejos para la tesis preparadas por los tutores de Docsity
CURSO DE EXODONTIA PARA ESTOMATOLOGIA
Tipo: Diapositivas
1 / 70

Esta página no es visible en la vista previa
¡No te pierdas las partes importantes!
ACCIDENTS AND COMPLICATIONS Dr. José María Aguado Dra. María Luisa Martínez Dr. Alberto Herranz
Clinical exam + X-rays
Prevention of Extraction of Wrong Teeth Focus attention on the procedure. Check with the patient and the assistant to ensure that the correct tooth is being removed. Check, then recheck, images and records to confirm the correct tooth.
Use Use surgical (i.e., open) extraction technique to reduce the force required. Do not use Do not use excessive force. Conduct Conduct thorough preoperative clinical and radiographic examinations.
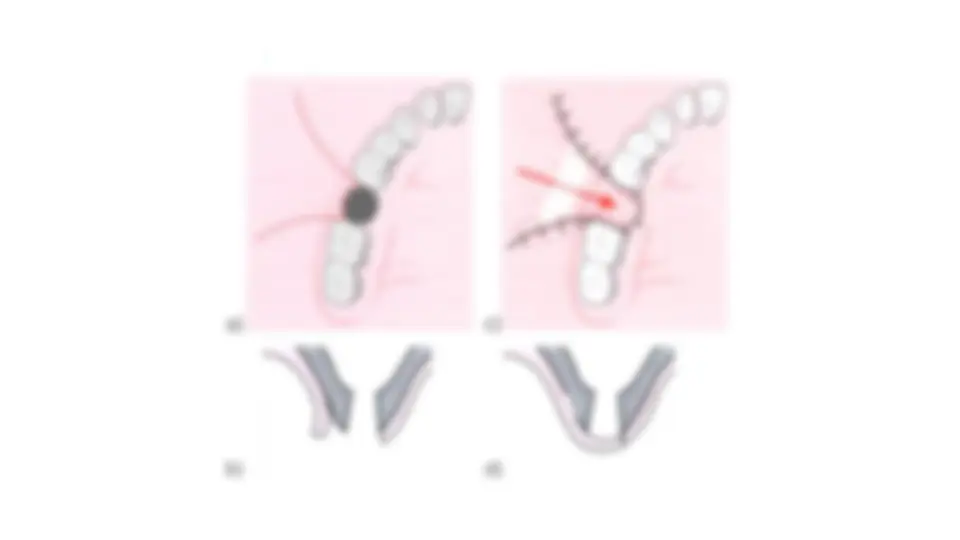
Complication of a large fracture of bone in the maxillary tuberosity
Complications: