


THE ENDOCRINE SYSTEM
1








Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
This shades a light on the endocrine system, and it helps you understand the Endocrine system
Typology: Study notes
1 / 14

This page cannot be seen from the preview
Don't miss anything!
General Function The nervous system and the endocrine system are the two main coordinating and controlling systems of the body. There are several differences between these two systems. For example, the nervous system acts by means of electric impulses and chemical stimuli; whereas the endocrine system has more widespread, slower, and longer lasting effects. The endocrine system also has more generalized effects on such activities as growth, metabolism, and reproduction. Despite this difference, however, the two systems are closely interrelated. Hormones The chemical messengers released by the glands of the endocrine system are called hormones. Hormones are released directly into the bloodstream and carried to the tissues they affect. These tissues may be far from where the hormone is produced. The blood reaches all cells of the body, but only certain cells respond to specific hormones; these responding cells are unique in that they have receptors to which the hormones attach. Only cells that have receptors for a given hormone will respond to that hormone; these cells make up what is called the target tissue. Chemistry Hormones fall chemically in two categories:
The endocrine system consists of the glands that secrete hormones. These glands are also called the ductless glands because they secrete directly into the blood stream, in contrast to the endocrine glands, which secrete into body cavities. Most endocrine glands, like exocrine glands, are made of epithelial tissue. Although they have no ducts, they have an extensive blood vessel network. Operations on endocrine glands, for example on the thyroid, require care in the control of bleeding. The organs believed to have the very richest blood supply of any in the body are the tiny adrenal, or suprarenal glands, which are located near the upper part of the kidneys. Some of the glands included in this system, such as the pancreas and the sex glands, have other non-endocrine functions as well, but hormone secretion is one of their main functions. In addition, some body organs, such as the stomach, small intestine, and kidney, produce hormones, but since their main function is not hormone production, they are not discussed. The Pituitary Gland The pituitary gland or hypophysis, formerly called the "Master gland", secretes several polypeptide hormones that directly or indirectly regulate a wide variety of metabolic and physiologic processes essential to normal growth and development as well as to the maintenance of homeostasis. Many of the hormones secreted by the pituitary gland are critical to the activity of target glands, including the thyroid, adrenal and gonads. Anatomy The pituitary gland (hypophysis cerebri) is located at the base of the brain, resting within the Sella turcica of the sphenoid bone. The pituitary gland maintains elaborate neural and vascular connections with the hypothalamus of the brain, which plays a central role in the integration of neuroendocrine activity. The pituitary gland has two major divisions: The anterior lobe (adenohypophysis) and the posterior lobe (neurohypophysis). The hormones released from each lobe are; Adenohypophysis: Somatotrophs , which secrete growth hormone (GH) or somatotropin. Lactotrophs , which secret prolactin (PRL). Corticotrophs , which produce corticotropin (ACTH) and beta-lipotropin (beta-LPH) Thyrotrophs , which secrete thyrotropin (TSH). Gonadotrophs , which produce follicle stimulating hormone (FSH) and luteinizing hormone (LH) Neurohypophysis: The neurohypophysis, which is connected directly to the hypothalamus by the infundibular (Pituitary) stalk, is rich in nerve fibers of hypothalamic origin (the hypotahlamohypophyseal tract) produce two hormones: A ntidiuretic hormone (ADH or Vasopressin) and oxytocin.
These hormones are then transported along the axons of the hypothalamo hypophyseal tract to the posterior lobe of the pituitary gland for storage and ultimate release under hypothalamic control. Hormones of the Adenohypophysis The secretion of hormones by the adenohypophysis is controlled by hypothalamic regulatory (hypophyseotropic) hormones that are transported to the pituitary gland by the hypothalamohypophyseal portal system. There are six recognized hypophyseotropic hormones secreted from the median eminence of the hypothalamus:
Oxytocin: The two major physiologic actions of oxytocin are exerted on the female breast and uterus. Actions It causes uterine contractions and triggers milk ejection from the breast. The ejection of milk from a lactating mammary gland follows a neuroendocrine reflex initiated by sucking, which stimulates cutaneous receptors in the areola of the breast. Oxytocin is carried by the blood to the mammary gland, where it causes contraction of myoepithelial cells surrounding the alveoli and lactiferous ducts to bring about the ejection of milk (milk letdown). In lactating women, tactile stimulation of the breast areola, emotional stimuli, and genital stimulation may also lead to oxytocin release and activate the ejection of milk. It also acts directly on uterine smooth muscle to elicit strong, rhythmic contractions of the myometrium. Uterine sensitivity to oxytocin varies with its physiologic state and with hormonal balance. The gravid (Pregnant) uterus is highly sensitive to oxytocin, particularly in the late stages of gestation. Uterine sensitivity to oxytocin is greatly enhanced by estrogen and inhibited by progesterone. Oxytocin release appears to follow a neuroendocrine reflex initiated by genital stimulation. It has been suggested that oxytocin may facilitate sperm transport through the female genital tract. The Thyroid Gland The hormones of the thyroid gland exert a wide spectrum of metabolic and physiologic actions that affect virtually every tissue in the body. Anatomy The thyroid gland is the largest of the endocrine glands. A bilobed ( two roughly oval lateral lobes on either side of the larynx connected by anarrow band called isthmus) its located in the neck overlying the trachea anteriorly. The thyroid gland is composed of numerous closely packed spheres or follicles. Each follicle consists of a simple cuboidal epithelium (follicular cells) enclosing a lumen or cavity containing a viscous hyaline substance termed colloid. The chief constituent of the colloid is the iodinated glycoprotein thyroglobulin. Interspersed among the follicles are small clusters of parafollicular (C) cells, which secrete calcitonin, a hormone affecting calcium metabolism. Thyroid Hormones The follicular cells of the thyroid gland secrete two hormones, thyroxine tetraiodothyronine or T4), triiodothyronine (T3). Storage and release of thyroid hormones : T3 and T4 remain stored within the colloid bound to thyroglobulin until a stimulus for secretion arrives. On stimulation by TSH, portions of the TGB (colloid) are engulfed by microvilli that extend from the apical surface of the follicular cells. Droplets of the engulfed colloid fuse with lysosomes, and proteolytic enzymes release T3 and T4 from the TGB. The hormones (T3 and T4) readily diffuse to nearby capillaries and enter the bloodstream.
Actions The thyroid hormones increase the rate of metabolism, total heat production, and oxygen consumption in most body tissues. Exceptions include the adult brain, spleen, lymph nodes, uterus, and testes. The thyroid hormones promote normal physical growth and development, and they are essential for normal myelination and development of the nervous system in early life. Hypothyroid infants exhibit severe mental retardation and defective myelination of nerve fibers. In normal physiologic amounts, the thyroid hormones stimulate protein synthesis, increase lipid turnover, lower plasma cholesterol, and promote GI absorption of glucose. T3 is more potent and more rapidly active than T4; in fact, the latter may be considered a prohormone, since most target cells convert T4 into T3. The Parathyroid Glands The parathyroid glands, usually four in number, are embedded in the dorsal surface of the thyroid gland. In response to hypocalcemia (low plasma calcium), the chief cells of the parathyroid glands secrete a hormone known as parathyroid hormone (PTH). Parathyroid hormone regulates serum calcium levels by exerting its effects on the following target tissues:
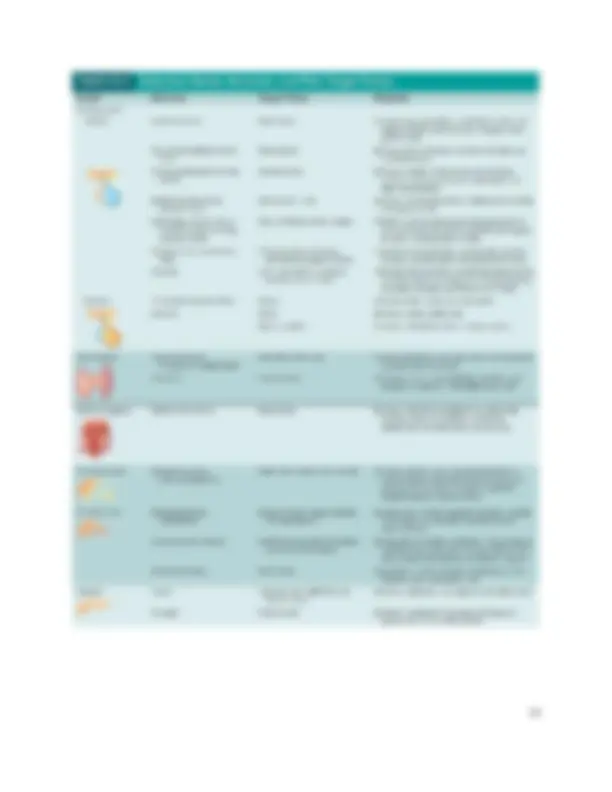
Major Actions
Actions of Adrenal Medullary Hormones Epinephrine and norepinephrine mimic the effects of sympathetic nerve discharge, producing the following effects:
substances from the hypothalamus, which may in turn regulate the secretion of gonadotropins from the pituitary. There is evidence from animal studies that the production of melatonin is regulated by the amount of light in the environment.