Download Pharmacy notes lesson and more Summaries Pharmacology in PDF only on Docsity!
ANTIDIABETIC DRUGS
REAGAN KABUKA (Bpharm, MPH)
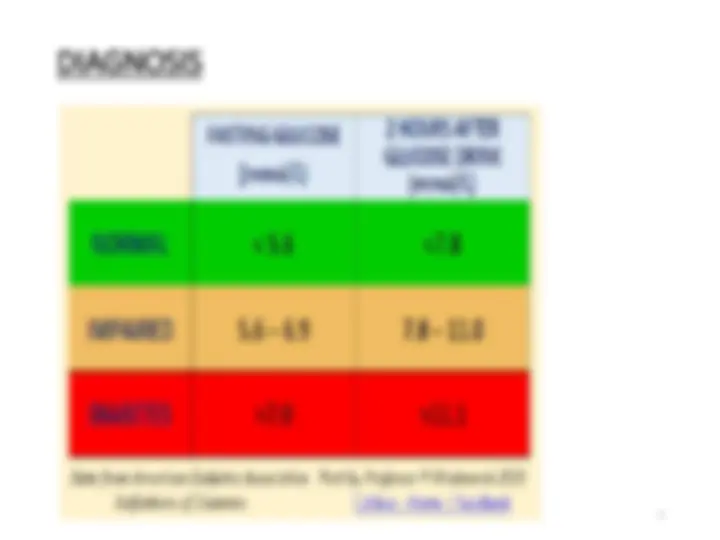
DIABETES MELITUS
DM is a metabolic disorder characterized by chronic Hyperglycaemia due to absolute or relative lack of insulin or due to insufficient insulin activity
CAUSES OF DM
- Primary DM; IDDM; destruction of beta cells (autoimmune) NIDDM; Insulin resistance or insufficient insulin release
- Secondary DM; due to either pancreatic, Hormonal disease (e.g. Cushing syndrome, acromegaly, Pheochromocytoma, Gestation (pregnancy induced) or drug induced
PATHOGENESIS
IDDM
- Auto immune antibodies are formed against the islets of Langerhans cells causing destruction of B-cells, thereby resulting into loss of insulin production.
- Drugs that suppress the immunity like cyclosporine may preserve the beta cells.
- This type is usually common in young people <30 years.
SIGNS AND SYMPTOMS
Tiredness Hyperglycaemia Frequent urination Increased thirst Blurred vision Weight loss Dehydration
MANAGEMENT OF DM
• TREATMENT GOALS FOR DM
To achieve near normal glycaemia. Minimise the occurrence of hyperglycaemia and hypoglycemia To reduce the risk for microvascular and macrovascular disease complications To improve symptoms, reduce mortality, and to improve quality of life.
INSULIN
- Insulin is secreted from the B-cells in the islets of langerhans of the pancrease
- Insulin is usually injected into the upper arms, thighs, buttocks, or abdomen
- Generally as subcutaneous insulin injections
- Fat hypertrophy occurs with this ROA, however, occur but can be minimised by using different injection sites in rotation
- Local allergic reactions are rare
Mechanism of insulin
- Insulin binds to a specific receptor consisting of two alpha and two beta subunits.
- The alpha subunits are extracellular and carry the insulin-binding site.
- The beta subunits span the cell membrane, its intracellular end has tyrosine kinase.
- Binding of insulin results in autophosphorylation of the tyrosine kinase. This causes activation of intracellular protein kinase affecting different metabolic enzymes e.g. phosphorylase, lipase
- The number of insulin receptors is increased by exercise and loss of weight
- The number of insulin receptors is decreased by excess insulin (down regulation), obesity and growth hormone
- The affinity of insulin to its receptors is decreased by glucocorticoid and oral contraceptives
INTERMEDIATE ACTING INSULIN;
- Onset 2 hours, duration 12 hours
- E.g. Natural protamine Hagedorn (NHP) LONG ACTING INSULIN
- Onset 3hours, duration 14-36hours
- E.g. Glargine, Detemir
INSULIN DOSING AND REGIMENS
- **Total Daily Insulin requirement (TDI) =0.55units/ kg
- ONCE DAILY REGIMEN**
- Intermediate acting insulin with or without short acting insulin – once a day at breakfast
Indication
• IDDM
• DKA
- NIDDM after failure of diet control and full doses of sulphonylureas
- DM during pregnancy and lactation
- Treatment of hyperkalaemia
- Patients with severe renal or hepatic disease
Side effects
- Hypoglycaemia
- Insulin Allergy
- Redness, swelling and itching at the site of injection
Signs and Symptoms
- Polyuria
- Vomiting
- Abdominal pain
- Dehydration
- Hyperventilation
- Coma
Treatment of DKA
- Adequate Fluid replacement (3-5L) isotonic saline
- 5% glucose if the BG drops to 14mmol/L to avoid brain damage
- Insulin therapy continuous IV infusion 0.15units/kg/hour. Reduce to half when the blood glucose levels reduce to 14mmol/L
- Potassium replacement , if normal potassium levels, give 20mmol/L, if there is hypokalaemia give 40mmol/L
- Bicarbonate therapy is indicated in severe acidosis (pH< 7.1) and should be stopped when pH reaches 7.2.