Approach to
Electrocution
Presented by:
Sweta Ghimire
MBBS 14th Batch
Date:2082/09/15
General Practice and Emergency
Medicine
Objectives:
●Define Electrocution
●Classify Electrical injury
●Understand Pathophysiology
●Emergency approach and management
●Identify patient for admission vs discharge
Loading…
Introduction:
•Definition: Electrocution = injury caused by
electric current passing through the body.
• Can cause cardiac arrest, burns, neurological
injury, and death.
•Epidemiology:
• Common in occupational (construction,
electricians) and domestic settings
• Children at risk at home.
•High-voltage exposure (>1000 V)-↑Mortality
Why Electrical Injuries are Unique?
●Small skin burn ≠ small internal injury
●Can cause sudden cardiac arrest
●Delayed complications common (arrhythmias,
neuro deficits)
●Requires observation even if patient looks fine
Loading…
Classification of Electrical Injuries
❑Based on Voltage
•Low voltage: <1000 V
•High voltage: >1000 V
• More severe injuries
• Higher risk of cardiac arrhythmias, deep tissue
damage, and mortality
❑Based on Type of Current
•AC (Alternating Current):
• More dangerous
• Causes tetanic muscle contractions
• Victim unable to let go → prolonged exposure
•DC (Direct Current):
• Causes a single strong muscle contractor
• May throw the victim away from the source
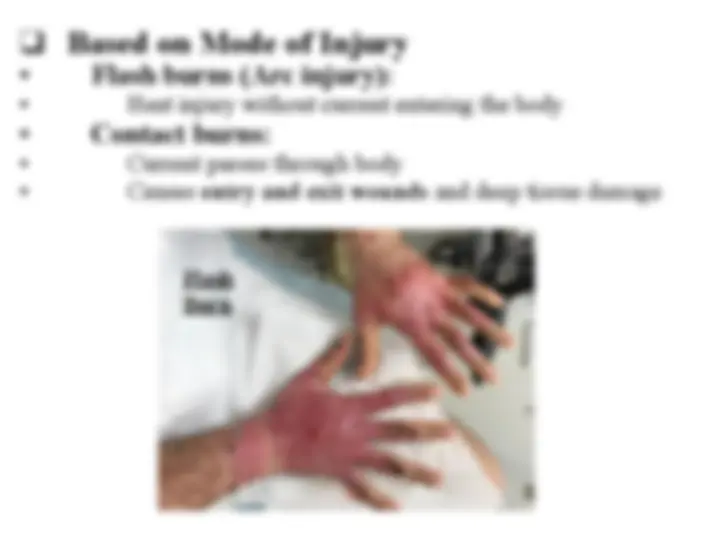
❑Based on Mode of Injury
•Flash burns (Arc injury):
• Heat injury without current entering the body
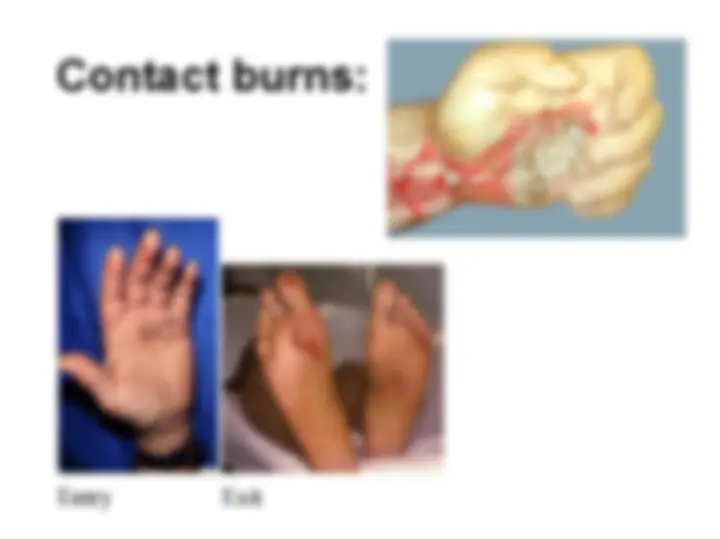
•Contact burns:
• Current passes through body
• Causes entry and exit wounds and deep tissue damage
Flash
Burn
Contact burns:
Pathophysiology:
• Electric current → tissue injury via:
•Direct thermal injury → Burns
•Electroporation → cell membrane damage
•Cardiac effects → Arrhythmias, Asystole, VF
•Neurological effects → Direct nerve damage,
Demyelination, Ischemia
•Musculoskeletal → Fractures,
Rhabdomyolysis
Loading…
Management:
Pre hospital Consideration
• Ensure scene safety first
• Power source off
• Reverse triage principle (lightning/mass
casualty)
• Treat patient appearing dead first
• Then attend those with signs of life
• Early CPR and ventilation
Primary Survey (ABCDE)
A – Airway ± cervical spine
B – Breathing give O₂ if needed.
C – Circulation
• Check pulse, BP
• Monitor ECG for arrhythmias (VF, VT, asystole)
• Start IV access and fluids
D – Disability: GCS, pupil,glucose
E – Exposure: Complete undressing, assess burns,
prevent hypothermia.
Airway and breathing
• Airway burns or
inhalational injury
• Altered sensorium (GCS ≤
8)
• Respiratory failure
• Cardiac arrest / severe
arrhythmias
• Associated head or
cervical spine injury
Indications For Intubation
Cardiac consideration
•VF, VT, asystole
common
•Continuous cardiac
monitoring
•ACLS protocol if
cardiac arrest
•Pupils unreliable in
lightning injury
Secondary Survey
•History:
• Voltage & duration of exposure
• AC vs DC
• Entry and exit wounds
• Witnessed cardiac arrest
•Examination:
• Burns – entry & exit wounds
• Neurological deficits
• Musculoskeletal injury
• Renal assessment (dark urine → rhabdomyolysis)
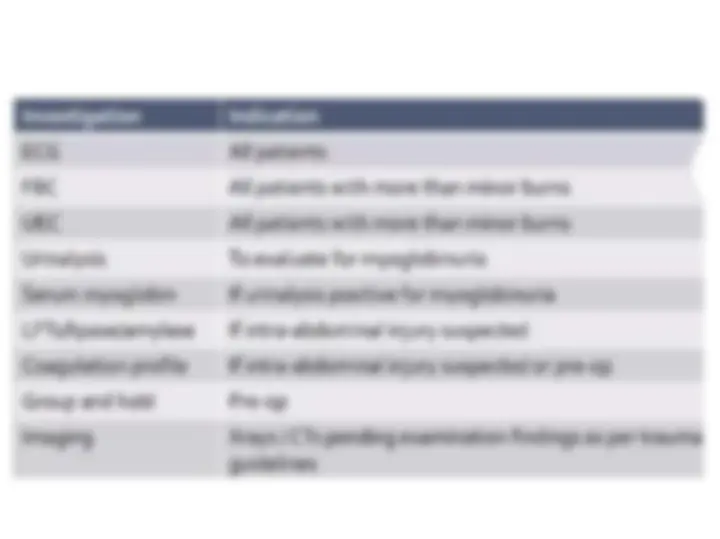
•Blood tests: CBC, electrolytes, renal function, CPK
(muscle injury), troponin
•ECG: Look for arrhythmias, conduction
abnormalities
•Urine: Myoglobinuria → rhabdomyolysis
•Imaging: X-ray for fractures, CT if CNS injury
suspected
•Other: Cardiac monitoring for 24–48 hours in high-
voltage injuries
Monitoring and Investigations
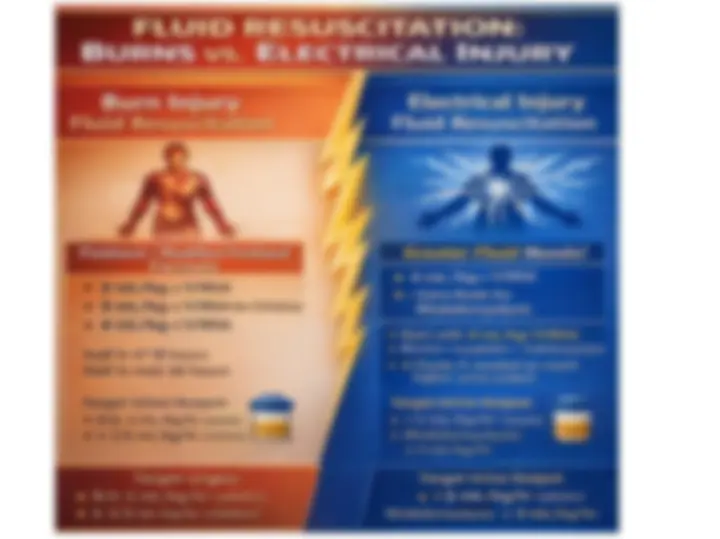
Injury and Burn Care
●Cover large burns with dry sterile dressings
●Clean & treat minor burns routinely
●Fluid resuscitation (Parkland’s formula if >10%