Download Physiotherapy 2 note lecture study and more Lecture notes Physiotherapy in PDF only on Docsity!
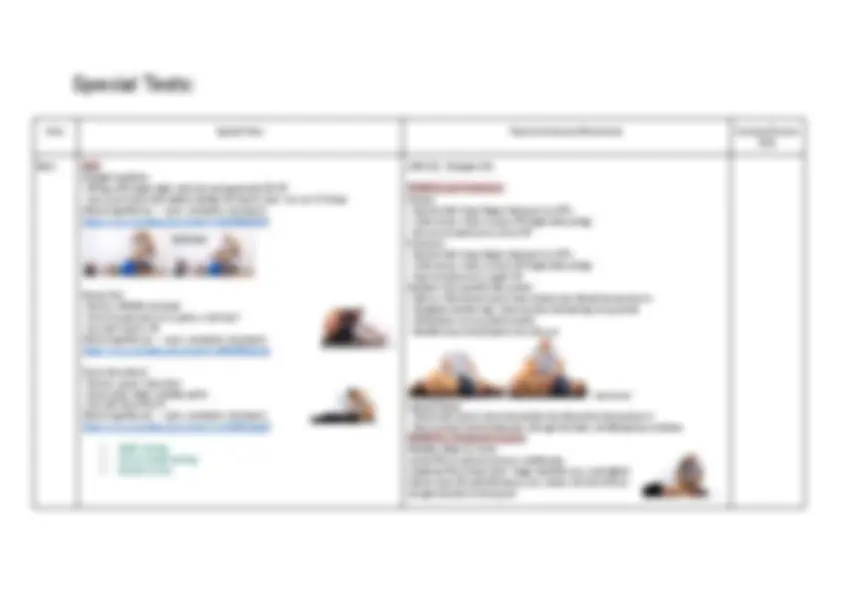
AROM + OP:
Movement Testing position Distal landmark Axis of rotation Proximal landmark Image
Back Flexion (60°)
Standing, flexes forward Measure fingers to toes
Back Extension (25°)
Standing in front of plinth, PT on plinth behind pt, pt extends backward
Back lateral flexion (25°)
Standing, pt bends to side
Hip Flexion (140°)
Supine, both knees extended, hips and pelvis neutral lateral midline of the femur
lateral aspect of hip joint lateral midline of pelvis
Hip Extension (15°)
Lying prone with both knees extended and hips neutral. No pillow under head, but thin pillow may be placed under abdomen for comfort
lateral midline of the femur
lateral aspect of hip joint lateral midline of pelvis
Hip Abduction (45°)
Supine with knees extended and hips neutral. Position patient at the edge of plinth opposite to the limb being tested, to allow the table to support limb
anterior midline of the femur
anterior superior iliac spine (ASIS) of the extremity being measured
horizontal line extending from one ASIS to the other
Hip Adduction (25°)
Supine with knees extended and hips neutral. Abduct the opposite hip to the one being tested (slightly), to allow for full ROM
anterior midline of the femur
anterior superior iliac spine (ASIS) of the extremity being measured
horizontal line extending from one ASIS to the other
Hip Internal Rotation (45°)
Seated with hips and knees flexed at 90 degrees anterior midline of the lower leg
anterior aspect of patella perpendicular to the floor
Hip External Rotation (60°)
Supine with hip and knee flexed at 90deg anterior midline of the lower leg
anterior aspect of patella perpendicular to the floor
Knee Flexion (140°)
Lying supine with knee in full extension, hip neutral (towel can be placed under ankle to ensure full extension)
midline of the fibula lateral epicondyle of the femur
lateral midline of the femur
Knee Extension (5°)
Lying supine with knee in full extension, hip neutral (towel can be placed under ankle to ensure full extension)
midline of the fibula lateral epicondyle of the femur
lateral midline of the femur
Ankle Dorsiflexion (25°)
leg hanging off plinth, the foot should be at 0 degrees inversion/eversion lat aspect of the 5th metatarsal
lateral aspect of the lateral malleolus
lateral midline of the fibula Opp way to below
Ankle Plantarflexion (40°)
leg hanging off plinth, knee at 90 degrees flexion, the foot should be at 0 degrees inversion/eversion
lat aspect of the 5th metatarsal
lateral aspect of the lateral malleolus
lateral midline of the fibula
Ankle Inversion knee flexed at 90 degrees, lower leg hanging off plinth ant midline of the 2nd metatarsal
anterior aspect of ankle midway between malleoli
anterior midline of lower leg
Ankle Eversion knee flexed at 90 degrees, lower leg hanging off plinth ant midline of the 2nd metatarsal
anterior aspect of ankle midway between malleoli
anterior midline of lower leg
Opp way ^
Hip + SIJ Hip Tests: Quadrant
- Passive into flexion, cradle leg, wide stance
- IR, take in across to adduction
- stabilise pelvis with trunk
- put body weight on knee and push down and scoop → pain in groin (acetabulum impingement) https://www.youtube.com/watch?v=xyJUIhsL4lg FABER - supine, cross leg over other leg above knee
- Make sure ankle is free and not supinating
- Fixate opposite ilium, slowely lower knee to bed Clinical significance → pain https://www.youtube.com/watch?v=89Qiht82zmg Thomas Test/Modified Thomas Test - supine; bring knee as far to the chest as possible and to hold it afterwards
- Ask: if they can feel a stretch in the groin → clinical significance: leg lifting off table Modified Thomas Test: GT on edge of plinth, head on pillow, increase hip flexion if lumbar hyperextension is present, → Abducts - tight ITB, or knee will extend - tight rectus femoris Always help patient up from modified position https://www.youtube.com/watch?v=NMDd-4NspHs Ober’s Test
- Side-lying neutral, knees flexed
- Push down on top of ilium
- Passively add/E leg → see where leg wants to stop (tight ITB) Nobles test in Obers position, palpation of lateral epicondyle https://www.youtube.com/watch?v=Amjv6FzDeLE Derotation test
- Pt in supine
- Position affected leg in 90deg flexion
Caudad (neutral or 90° flexion) (with or without belt/your choice)
- 90deg Hip F, using padding on pt before placing belt, belt goes around thigh of pt and below sacrum of pt
Lateral glide (with or without belt/your choice)
- In step stance, leaning away with body weight, take slack up by holding ankle with both arms - wither sustain or oscillate (do not do full body oscillation, only oscillate at end range for 30sec)
Flex: AP glide on femur Ext: PA
- Externally rotate the hip
- Have pt actively IR against resistance back to neutral
- Can repeat in prone → Look for reproduction of groin pain https://www.youtube.com/watch?v=nwBnc3I53QY Adductor Squeeze test
- pt squeeze fist with knees extended and flexed
SIJ Tests: Sacral Thrust
- Grip with pisiform on SP, 5-10s force perpendicular to sacrum
Thigh Thrust
- Hip 90def F, slight add, lean in with BW for 3-5s, palpate line of SIJ, compress along femur
- feel for clunk in soft tissue
Compression
- compress on outside of iliac crest, ASIS, in line with coronal plane Distraction
- Hands crossed inside with gap on ASIS
Active SLR + compression
- lift leg to about 30deg
- SLR with compression is easier, → perception of heaviness
Knee Patella
Patellar Dynamic Apprehension
- translate patella laterally while leg extended to flexion
- pt SOEOB → reproduce pain https://www.youtube.com/watch?v=IKhEElT8jvQ Patellar Grind Test
- Relax, push patella down, get pt to tighten quads
TFJ: AP, PA - prone, foam roller under ankle, web space around popliteal space and push PFJ: Med, lateral, cephalad, caudal glides, med/lateral tilt
https://www.youtube.com/watch?v=JlhydJhF-5U
Flexion: AP glide on tibia Extension: PA glide on tibia
LCL
Varus Stress Test (0◦ or 30◦)
- rotate body away from midline, avoid hip rotation → gapping by palpating LCL https://www.youtube.com/watch?v=sg1gk6QKARw
MCL
Valgus stress Test (0; secondary stabilisers or 30◦: primary stabiliser )
- rotate body towards from midline, avoid hip rotation → gapping by palpating MCL
https://www.youtube.com/watch?v=QX1iLSc1TVA
Meniscus McMurray’s Test
- IR tibia, flex knee, move around in circles each way, then do again ER tibia
- avoid hip R → meniscus pain/click/lock https://www.youtube.com/watch?v=lwDFPAyGGgI
Lat Men Med Men Apley’s Test
- Prone, knee F, ER tibia, apply force along shaft of tibia → meniscus pain/click https://www.youtube.com/watch?v=6Z_9lfX_Pc Thessaly’s Test - SLS, flex knee to twenty deg and rotate side to side
→ meniscus pain/click Dial Test
- Prone, 30deg knee F, max DF, ER heels → PLC
- Repeat at 90deg → PLC & PCL https://www.youtube.com/watch?v=3UGffd71KyI Fractures Ottawa knee rules (fractures)
- aged 55 years or over.
- tenderness at the head of the fibula.
- isolated tenderness of the patella.
- inability to flex knee to 90 degrees.
- inability to bear weight immediately and at presentation.
Ankle ATFL
Anterior Drawer
- knee F, grip malleolar + calcaneal, pull calcaneal forward → pain https://www.youtube.com/watch?v=vAcBEYZKcto CFL - neutral / ATFL - PF / PTFL - DF Talar Tilt
- palpate respective ligament, grip malleoli + calcaneal, tilt calcaneus → pain https://www.youtube.com/watch?v=UHNbm6Z3XK Deltoid Reverse Talar Tilt
- palpate respective ligament, grip malleoli + calcaneal, tilt calcaneus Syndesmosis Lunge +/-Compression Test (syndesmosis, less painful with squeeze
- lunge on plinth, then repeat lunge and squeeze → reduced pain over syndesmosis https://www.youtube.com/watch?v=GnRVUOQF7mA Foot External Rotation + DF Test (syndesmosis)
- Sitting, maximal DF, ER tibia
TCJ: AP, PA, distraction: supine stabilise foot into DF with body
STJ: med, lateral glides: side lying, stabilise foot with body Top leg with roller Side lying bottom leg https://www.youtube.com/watch?v=v7D57FzVM4w
Regress: split stance with toe touch, ↑ bed height, Iso hold Progress: SL sit to stand, jumps + changing direction Feedback: palpate, biofeedback Dosage: until fatigue Adjuncts: tens, ice, biofeedback, soccer education, training with no pain Case 3: (L) ankle sprain A 60 year old female sustained a (L) ankle sprain (plantarflexion/inversion) in a low energy injury 3/52 ago. The condition is resolving however she still reports minor pain (2/10) after walking for 30mins. She is also worried about her condition as she does not want to injure the ankle again and is hesitant to return to her aquarobics class and social dancing.
Objective examination findings:
- Observation: Minor lateral ankle swelling
- Palpation: Minor tenderness over ATFL
- Move: Full active ankle plantarflexion, dorsiflexion, inversion and eversion. Minor pain into combined dorsiflexion and eversion.
- Balance: Poor (L) single leg stance – unsteady, clawing toes as compensation and using arms to counter balance. However is able to maintain (L) leg single leg balance for equal amount of time as (R).
Aim: improve balance Exercise: Fix clawing in SLS then do compass + clicking while touch chair Regression: SLS with touch + reaching out of BOS Progress: no chair, nutbush (home exercise through nutbush at home) Feedback: tape on floor Dosage: until fatigue Adjuncts: analgesic, ice
Case 4: (L) anterior knee pain A 33 year old woman reports gradually increasing (L) anterior knee pain. It does not currently restrict her activities however the pain as been increasing in intensity and frequency. She is normally sedentary at home and works part-time at a shop where she stands for long periods (4-5 hours). The pattern of aggravation is variable often with the pain getting out of a car, getting up from sitting in the lounge at home or getting up from kneeling on the floor.
Objective examination findings:
- Observation: Poor muscle bulk bilaterally; increased Q angle ((L) & (R)) Valgus knees
- Palpation: No significant finding; Minor synovitis on swipe test ((L) = (R)) Equal on both sides Move:
- Strength: Knee extension & flexion (L) = (R) (both 4/5) Function:
- Step up: Pain+ after 10 repetitions on (L) and not painful on (R) Aim: ↑ strength Exercise: Sit to stand with split stance R) behind (L) Regress: SL leg extension, Isometric hold Progress: turn to R and stand → Getting out of car (height, angle) Adjunct: pacing (sit down every 15minutes), education, ice, analgesia, activity medication (add height to chair), activity modification out of car (swing both legs out) Dosage: until fatigue, during work, morning/ night
Case 5: hamstring A 35 year old man reports (R) hamstring soreness after playing soccer with his young children 4 days ago. He is a keen golfer and reports feeling the discomfort when playing golf, especially when setting up into his stance at the tee. The pain does limit his golf swing as he tries to avoid feeling the pain. He also reports feeling some tightness towards the end of a round of golf, possibly as he has had to walk for a prolonged period.
Objective examination findings:
- Observation: nil significant
- Palpate: Tender to palpate over mid-belly of (R) hamstring muscle group Move:
- Muscle strength: (R) is 90% (3/10 pain) of (L) (hand-held dynamometer)
- Muscle length (SLR test): (L) = 60; (R) = 50° (P1 2/10)
- NTPT:SLR: (L) = 60°; (R) = 50° (4/10 pain with ankle dorsiflexion)
Aim: Increase strength in the same direction as the fibres without pain Exercise: Hamstring bridge on heels Regress: hamstring curls standing or sideways Progress: bridge on chair, (slide hands down legs to see where pain is - range) RDLS, Golf Feedback: no pain, Dosage: until fatigue Adjuncts: ice, education nerve (dont hunch, look forward, dont want to aggravate), proper form, tape, rest
Case 6: ankle reco A 25 year old netballer had a (L) ankle reconstruction (stabilisation) following a history of recurrent ankle sprains. Six weeks in a cam boot followed by 8 weeks of rehabilitation to recover ankle ROM and strength have allowed her to return to activities of daily living and work (sedentary) with no report of symptoms (pain/giving way). She is keen to progress to netball.
Objective examination findings:
- Observation: scar is well healed over (L) lateral ankle
- Palpate: Nil tenderness over scar or ankle.
- Move: AROM & Strength
- Ankle eversion: (L) = (R) and firm end feel with O/P and 5/5 or both
- Ankle inversion: (L) is ¾ of (R) and firm end feel with O/P and 5/5 or both
- Ankle dorsiflexion & plantarflexion: (L) = (R) both are 5/ Function
- Double leg jump and single leg land – apprehensive and hesitating to jump to same height when has to land on (L) compared to ®
- Running and cutting (left and right) – not pushing off as hard (reduced (R) step length) from (L) to go to right.
Aim: increase strength to return to sport ( ↑ strength of peroneal muscle) Exercise: Push of L) and land on R Regression: push of L) and land on both legs Progression: push of L) then land + push off R) quicker + catch a ball
- Regress this by reducing jump
Progress: to sitting (cant sit long periods of time), standing (taping, string through body, hand on hips, mirror), against wall with ball + step the heel strike, neutral in running (video) Feedback: taping, hands on hips, hand below back Dosage: little and often (good technique until failure, multiple times a day) Adjunct: heat, taping for posture, tens, analgesia, pillow prevent tilting
Case 9: Menisectomy A 40 year old male had a (R) knee menisectomy 3/52 ago. He had the arthroscopy as a result of 5 years of ongoing pain that had gradually become worse over the past 6 months. H was previously active participating in team sports and running regularly. He has been advised by his surgeon to avoid high impact activities as these may lead to knee pain due to degenerative changes that are present (chondral wear on femoral surfaces). He has progressed well so far 3/52 following his arthroscopy and reports only changing direction as causing minor discomfort (eg. getting in/out of car or putting weight on (R) leg as you change direction).
Objective examination findings:
- Observation: quadriceps bulk on (R)
- Palpate: Minor tenderness+ over medial femoral condyle (assessed in 90° knee flexion)
- Move: AROM:
- Knee extension: (L) = (R) = 0° (no pain & firm EF)
- Knee Flexion: (L) = 130° (springy EF); (R) =110° (2/10 pain & firm EF) Function:
- Walking gait: normal
- Step ups: (L) = 30 reps; (R) = 30 reps (reports minor discomfort in knee (2/10))
Aim: Increase ROM Exercise: Assisted AROM using other foot (on chair, bend foot back lean forward) Regress: Assisted AROM, no leaning forward Progress: Add load, lunge onto plinth (add in strength), Feedback: Adjuncts: activity modification out of car (swing both legs out), ice Dosage: little and often (ROM), to failure (strength)
Aim: ↑ Strength functionally Progress: sit to stand, add twisting component (reduce range) → stepping out of chair Regress: ↑ chair height
Case 10: LBP A 39 year old male reports LBP 10/7 ago following painting his ceilings at home. He felt pain the day after painting that has not eased since. He has trialled NSAIDs and analgesics for 5 days with no effect. He had one previous episode of LBP 3 years ago and has been performing the exercise taught to him. This exercise was extending the lower back in lying by pushing up onto his hands. He has continued with this exercise even though it has been increasing his pain while performing the exercise. His pain is low to moderate irritable, in that it may be severe but eases relatively quickly.
Objective examination findings: Observation:
- Standing posture – Keeping very upright (bracing with abdominal muscles)
- Sitting – Keeping very upright avoiding rotation and lateral flexion Palpation: Tender++ with unilateral Pas - L4/5 & L5/S1 ((L)=(R)) Move:
- Lumbar Flex – Minor tightness in lumbar region
- Lumbar Ext – Pain+ (P = 4/10)
- Lumbar LF – (L) = (R) (P = 2/10)