Download Physiotherapy 3 note lecture study and more Study notes Physiotherapy in PDF only on Docsity!
ANATOMY &
BIOMECHAN
ICS
TUTORIAL
- Address questions from Prep work
- Some questions may be saved for the PT S&P session for context reasons
- Open Q&A in prep for PT science and practice session
- Will need to sign on to mentimeter: - www.menti.com - Code: 5769 7518
APPLICATI
ON
- (^) Reflecting on the closed packed position of the hip, what are the potential clinical implications of this during typical movements and traumatic movements? Hints: propulsion + dislocation
- (^) What would be an abnormal/pathological end feel in the hip?
- (^) What would you expect an OA end feel to be? E.g. spasm
- (^) What would you expect a labral tear to be?
SELF
TEST
Limited Flexion Limited Abd Limited IR Osteokinematic (AROM/PROM) AROM, AAROM or PROM into flexion +/- hold relax of agonist or antagonist muscle. Arthrokinematic (PAM) Distraction Inferior glide -start in neutral and then progress to point of restriction Posterior glide -start in neutral and then progress to point of restriction. Myofascial (muscles that affect the movement of the joint) Stretches, STR, acupuncture, dry needling etc. to address the muscles that may be limiting the restriction
How would you address the following hip restrictions?
SAMPLE MCQ VERSION 1 Tim presents with left hip OA. He has pain and stiffness when sitting for prolonged periods of time, walking or standing. His movement loss is consistent with the capsular pattern of the hip. Which joint mobilization would be most appropriate. a) Traction b) Distraction c) Inferior glide d) Posterior glide
SELF TEST: TIBIOFEMO RAL JOINT CLASSIFICA TION The Tibiofemoral joint is (choose all that apply): A. Synovial B. Compound C. Complex D. Bicondylar, Modified Ovoid E. Modified Sellar F. Simple
SELF TEST:
TIBIOFEMORAL
JOINT
- (^) How many degrees of freedom?
- (^) What are these movements?
- (^) How would you describe the osteokinematics of these
movements?
- (^) What plane(s) does it move in? and about what axis?
COMPARE & CONTRAST
- (^) What is the pain pattern of the hip vs the knee?
- (^) How does an articular condition present in both?
- (^) How does a ligamentous condition present in both?
- (^) How does a muscular condition present in both?
- (^) How would you classify the hip joint?
- (^) How would you classify the knee joint?
- (^) Implications for manual therapy?
Hip Joint: Factors that affect biomechanics Excessive Anteversion with In Toeing = Serves to direct the femoral head more directly into the acetabulum Q: In what populations would you expect to see this and why? Q: What is the affect of the increased internal rotation on the hip muscles? Q: What would be the goals of Physiotherapy intervention?
Putting it all together:
Clinical Implications
IDEAL STANDING
POSTURE
What is ideal?
For who?
When in their lives?
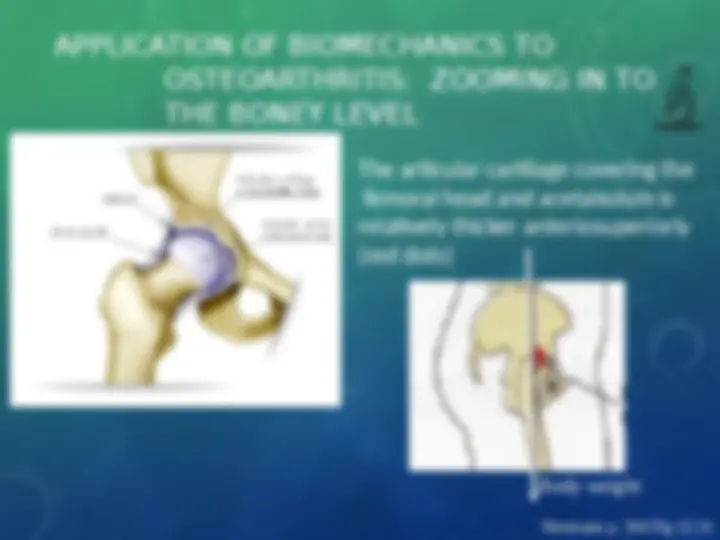
APPLICATION OF BIOMECHANICS TO OSTEOARTHRITIS: ZOOMING IN TO THE BONEY LEVEL The articular cartilage covering the femoral head and acetabulum is relatively thicker anteriosuperiorly (red dots) Body weight Neumann p. 504 Fig 12.
HIP JOINT: CAPSULAR PATTERN With early articular changes, pain may be present before articular changes are significant enough to cause a restriction in ROM
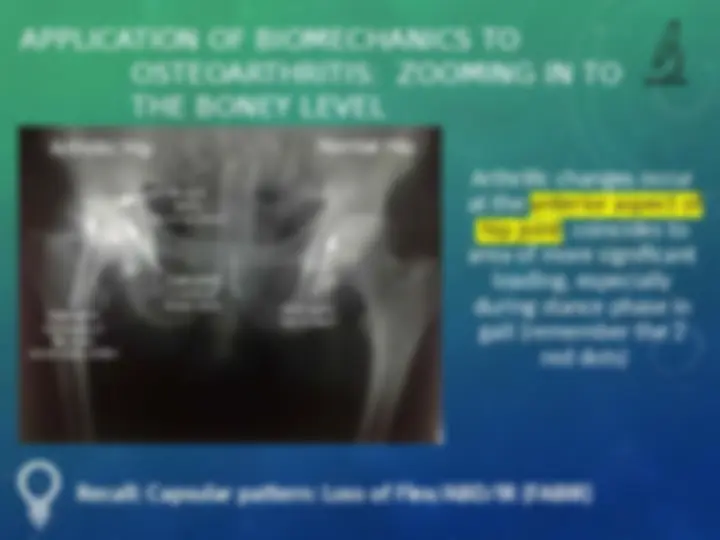
- (^) As a compensatory strategy , stride length is shortened to decrease stance time on the affected side to decrease pain. Body weight
As a compensatory strategy , stride length is shortened to decrease stance time on the affected side to decrease pain.
- (^) Clinically in early OA the presentation is a loss of
extension/IR and a restriction into flex/add and
extension/abduction quadrants (pain sensitive
structures are not as compressed)
- (^) As articular changes progress, to more moderated then
more marked/severe changes there is a gradual
progression in the pattern of movement loss
- (^) With advanced OA will see loss of Flex/ABD/IR (FABIR);
moderate extension loss and ER is usually spared (ie: OK)
Putting it all
together:
Clinical
Implications