


Pneumonia





























Studia grazie alle numerose risorse presenti su Docsity

Guadagna punti aiutando altri studenti oppure acquistali con un piano Premium

Prepara i tuoi esami
Studia grazie alle numerose risorse presenti su Docsity
Prepara i tuoi esami con i documenti condivisi da studenti come te su Docsity
Trova i documenti specifici per gli esami della tua università
Preparati con lezioni e prove svolte basate sui programmi universitari!
Rispondi a reali domande d’esame e scopri la tua preparazione
Riassumi i tuoi documenti, fagli domande, convertili in quiz e mappe concettuali
Studia con prove svolte, tesine e consigli utili
Togliti ogni dubbio leggendo le risposte alle domande fatte da altri studenti come te
Esplora i documenti più scaricati per gli argomenti di studio più popolari
Ottieni i punti per scaricare
Guadagna punti aiutando altri studenti oppure acquistali con un piano Premium
polmonite ambulatoriale polmonite ambulatoriale
Tipologia: Esercizi
1 / 50

Questa pagina non è visibile nell’anteprima
Non perderti parti importanti!
An HIV+ patient with a CD-4+ count of 802 is found to be hypoxic on room air. Chest X-ray shows multi-lobular consolidation. What is the most likely causative organism? A. Moraxella catarrhalis B. Klebsiella pneumoniae C. Staphylococcus aureus D. Streptococcus pneumoniae E. Mycobacterium tuberculosis Pre-Test
A 47 year old homeless alcoholic male presents to your clinic complaining of insidious onset dry cough. He describes his sputum as “red jelly.” Chest x-ray shows a bulging fissure. What is the most likely diagnosis? A. Aspiration Pneumonia B. Acute Bronchitis C. Ventilator Associated Pneumonia D. Hospital Acquired Pneumonia E. Adult Respiratory Distress Syndrome Pre-Test
A 47 year old homeless alcoholic male presents to your clinic complaining of insidious onset dry cough. He describes his sputum as “red jelly.” Chest x-ray shows a bulging fissure. What is the most likely diagnosis? A. Aspiration Pneumonia B. Acute Bronchitis C. Ventilator Associated Pneumonia D. Hospital Acquired Pneumonia E. Adult Respiratory Distress Syndrome Pre-Test
A 62 year old male presents with a non-productive cough of 2 weeks duration. Physical exam reveals wheezing, rhonchi, crackles. The patient has a normal pulse in but a high fever. What type of pneumonia is most likely? A. Typical Community Acquired Pneumonia B. Hospital Acquired Pneumonia C. Atypical Community Acquired Pneumonia D. Ventilator Associated Pneumonia Pre-Test
An HIV+ patient who has a CD-4+ count of 52 presents with acute onset cough and fever. He does not take antiretroviral meds or TMP- SMX, is hypoxic on room air, and has a diffuse bilateral infiltrate on chest film. What is the most likely causative organism? A. Streptococcus pneumoniae B. Pneumocystis carinii C. Aspergillis fumigatus D. Coccidiodes E. Mucormycosis Pre-Test
An elderly man presents w/ pneumonia, GI disturbance, bradycardia, and hyponatremia. What is the most likely causative organism? A. Streptococcus pneumoniae B. Staphlococcus aureus C. Legionella pneumophilia D. Coxiella burnetti Pre-Test
An elderly man presents w/ pneumonia, GI disturbance, bradycardia, and hyponatremia. What is the most likely causative organism? A. Streptococcus pneumoniae B. Staphlococcus aureus C. Legionella pneumophilia D. Coxiella burnetti Pre-Test
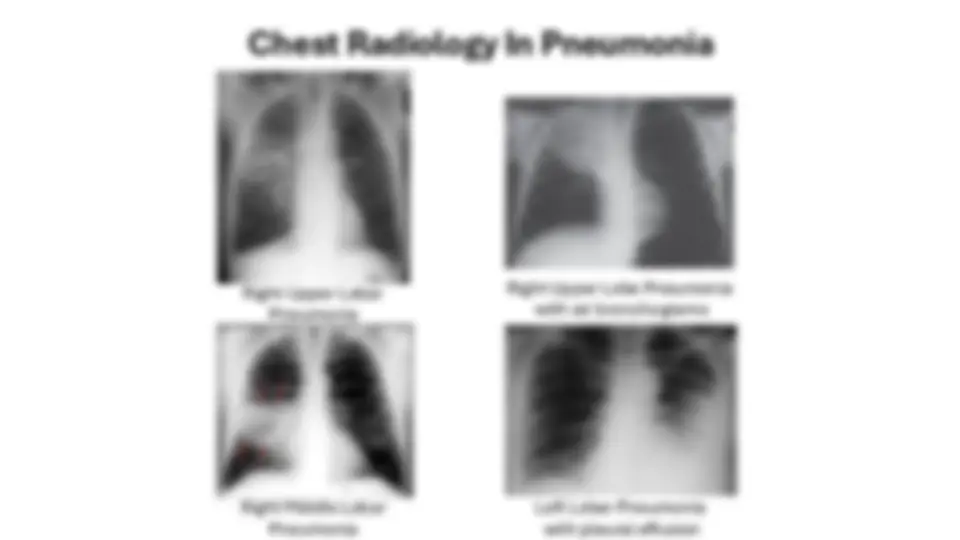
Left Lobar Pneumonia with pleural effusion Right Middle Lobar Pneumonia Right Upper Lobar Pneumonia Right Upper Lobe Pneumonia with air bronchograms