


























Estude fácil! Tem muito documento disponível na Docsity

Ganhe pontos ajudando outros esrudantes ou compre um plano Premium

Prepare-se para as provas
Estude fácil! Tem muito documento disponível na Docsity
Prepare-se para as provas com trabalhos de outros alunos como você, aqui na Docsity
Encontra documentos específicos para os exames da tua universidade
Prepare-se com as videoaulas e exercícios resolvidos criados a partir da grade da sua Universidade
Responda perguntas de provas passadas e avalie sua preparação.
Ganhe pontos para baixar
Ganhe pontos ajudando outros esrudantes ou compre um plano Premium
- - - - - - -
Tipologia: Notas de estudo
1 / 43

Esta página não é visível na pré-visualização
Não perca as partes importantes!
InsuficiênciaInsuficiência Aórtica Aórtica
EstenoseEstenose Aórtica Aórtica
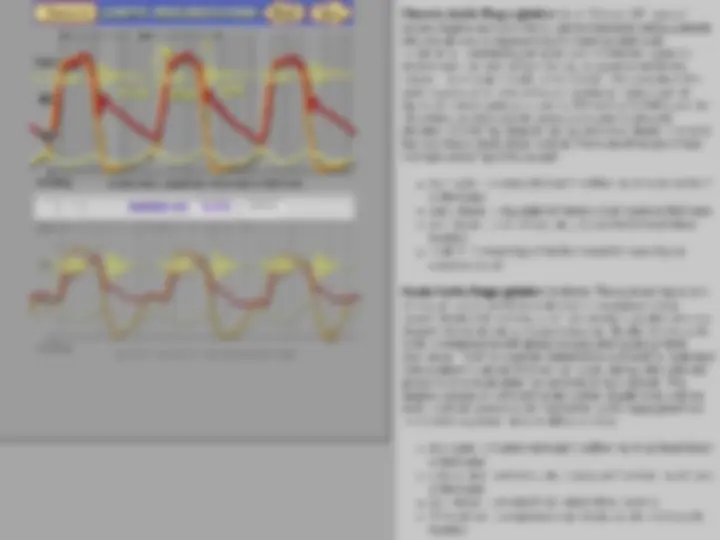
| Contents | FrontaliAnatomy. E Left atrium Left ventricle Aorta Right Atrium Right ventricle Pulmonary arteries Ribs Roll over list above to control animation. | Left Heart | -10 mmHg RA Watch the aortic and pulmonic valves, and listen, after clicking —— | Breathe ln Note the asynchronous valve closure, and the splitting of 82, as well as the delay, or "hangout" of the dicrotic notch on the PA pressure due to increased pulmonary compliance during inspiration, and the resulting delay of pulmonic valve closure (P2) Inspiration draws more blood into the night heart chambers (note their expansion) which increases right ventricular output into the more compliant lungs. Expiration inhibits right heart filling and enhances left heart filling by exerting positive pressure on the lungs. Integrating pulse with sounds and murmurs The carotid pulse in aortic regurgitation is prominent and may be seen upon approach to the bedside. When palpating the pulse, you will note the bounding character (a wide pulse pressure). A mid systolic dip may be palpable, due to high velocity flow (Venturi effect), resulting in a bisferiens (bro peaked) pulse Diastolic backilom through tha incompetent aortic valve causes a lower diastolic pressure in the aorta and increases the diastolic volume of the left ventricle, which in tum increases the stroke volume ancl systolic arterial pressure Compare AR with normal by clicking on the button below the animation The visibly bounding arterial pulse (Corrigan's pulse) may also be noted in peripheral sites, such as brachial and femoral arteries. In severe cases, head-bobbing (Musset's sign) and alternate blanching and reddening of the lighthy compressed nailbed (Quincke's pulse) may be seen Auscultation With the stethoscope diaphragm atthe 3rd left intercostal space GLICS), there are tero distinct murmurs (to-andro), separated by a pause, which represent the turbulent high velocity flow back and forth across the aortic valve. The increased aortic outflow causes a midsystolic murmur (MSM) ending well before 52. The regurgitant flow begins immediately with aortic valve closure, causing a blowing, decrescendo earty diastolic murmur (EDM) best heard in this area adjacent to the high-velocity regurgitant stream. tis helpful to have the patient sit up, lean fonvard, and exhale to bring out this often subtle murmur Moving the stethoscope over the ascending aorta (2RICS), will increase the systolic murmur's intensity. Alternating between 2RICS and 3UCS will bring out systolic (TO-fro) and diastolic (to- FRO) components, respectively EEE A0R7/C REGURGITATION; E Back Next d Sound at 3rd Left Intercostal Space [1 ») View Quincke's Pulse AORTIC REGURGITATION Austin Flint murmur Atthe apex, this patient demonstrates; * tachycardia (110 bpm) * a dynamic, displaced apical impulse * absence of 51” « A triple cadence consisting of * a midsystolic murmur * S2 initiating a brief earty diastolic murmur « a mid-diastolic (Austin Flint) murmur superimposed on the earty diastolic murmur, (to- fro-FRO). The large regurgitant volume rapidky expands the left ventricle, resulting partial or complete mitral valve closurs, impinging upon mitral inflowy. A rumbling, mic-diastolic Austin Flint murmur is best heard with the bell lightiy applied atthe apex Unlike the diastolic murmur at the base, the Austin Flint murmur starts well after 52. The resulting murmur combination should not be confused with a three-phase friction rub, which is scratchy and higher-pitched in quality In this patient, the presystolic component of the Austin Flint murmur is absent because of complete mitral valve preclosure *The character of 51 atthe apex is a useful diagnostic sign Torrential aortic backilow may overload the left ventricle, provoking premature closure of the mitral valve during diastole. Consequenily, 51 may be soft or absent. An absent S1, combined with an abbreviated early diastolic murmur, is asign of a poorly tolerated volume overload If'51 is split, the second component may be an ejection sound, resulting from the forceful flinging open of the aortic lgaflets Note: An exceptionalky loud, sharp sound initiating the micisystolic murmur in a patient with aortic regurgitation is usualky not the first heart sound, but an ejection sound caused by explosive aortic valve opening into a dilated aortic root. UA ADATIO REGURGITATION CHRONIC AORTIC REGURGITATION SOUND AT [3LICS | [ APEX Chronic Aortic Regurgitation (top): Chronic AR, even of severe degree as shown here, can be tolerated well by patients wino are able to compensate by increasing ventricular compliance, maintaining an open, non-constricted systemic arterial vascular bed, and producing a supernormal stroke volume. These adjustments can be made if the severity of the aortic regurgitation only increases gradual. In the example above, the aortic pulse pressure is 80 mmHg (120/40), and the left ventricular end diastolic pressure is only moderately elevated (20 mmHg) despite this patient's end diastolic volume thatwas nearly thres times normal, There are three prominent murmurs and a "split first sound": + mid systolic murmur (turbulent outflow murmur) heard best ai the base - early diastolic regurgitant murmur, best heard at the base + mid diastolic and presystolic (Austin Flinty mitral inflow murmur + "split 51" consisting of the first sound followed by an ejection sound Acute Aortic Regurgitation (bottom): The sudden imposition of a volume overload from acute aortic regurgitation may ovenhelm the left ventricle, as in this example, in which the end diastolic laft ventricular pressure rises rapidly after the diastolic nadir, overtaking the left atrial pressure and causing mitral preclosure. Time for diastolic mitral inflow is therefore restricted in this patient to about BO msec per cycle, during which the net stroke volume must enter the wentricle at high velocity. The diastolic pressure in the left ventricle then equilibrates with the aortic diastolic pressure, limiting further aortic regurgitant flow These hemodynamic abnormalities resultin + mid systolic murmur (turbulent outflowm murmur) heard best atthe base + abbreviated early diastolic regurgitant murmur, best heard atthe base + mid diastolic (Austin Flint) mitral inflow murmur + S1 is absent an ejection sound initiates the mid systolic mmurmur AORTIC REGURGITATION. E Back | Noxt Sound at 3rd Left Intercostal Space apdos ) ) I JUND ; il | EZES Adorno srenosis, E Baer | Hemodynamics and flow The murmur, outflom velocity, and transvalvar pressure gradient are interrelated because each represents manifestations (translations) of the underving pathophysiology of aortic stenosis. * the audible murmur results from high- velocity outflom through the narromed valve. + fonvard flow-velocity (away from Doppler probe at the cardiac apex) starts mhen the Ly and Ao pressures diverge, reaches a mid systolic peak of 5 Misec (equivalent to a gradient of 100 mmHg), and declines toward zero as the pressures converge tomard the end of systole. * the murmur ceases as fonward flow diminishes before reversing course to close the valve, there mill be a pause between the murmur and 52. * the duration of systole is prolonged, delaying AZ With more severe AS: » the LV pressure, and hence the gradient increases * the murmur peaks later