Download article-research clinical pharmacy and more Assignments Clinical Medicine in PDF only on Docsity!
[鍵入文字]
RESEARCH REPORT
SUBMITTED TO
CENTRE FOR HEALTH PROTECTION
DEPARTMENT OF HEALTH
General Public’s Knowledge, Attitude and
Practice Survey on
Antimicrobial Resistance 2016/
Submitted by
Social Sciences Research Centre
The University of Hong Kong
November 2017
Copyright of this survey report is held by the Department of Health
Table of Contents
Social Sciences Research Centre of The University of Hong Kong Page 3 of 172
Executive Summary
Introduction
The Department of Healthcommissioned the Social Science Research Centre ofthe
University of Hong Kong (“HKUSSRC”) to conduct a territory-wide telephone survey to
gauge the general public’s awareness ofAntimicrobial Resistance (“AMR”)problem;
knowledge, attitude and practice onantibiotic use; and their views on potential control
measures and AMR-related health promotion.
Research Methodology
The survey was an anonymous telephone survey conducted usingthe Computer Assisted
Telephone Interviews (CATI). The sample was drawn randomly from a list of telephone
numbers, which included unlisted and new numbers. The target respondents were
Cantonese, Putonghua or English-speaking non-institutional Hong Kongresidents
(excluding foreign domestic helpers) aged 15 or above. A bilingual (Chinese and English)
questionnaire was used to collect data.
Fieldwork took place in the call-centre of HKUSSRC on all the weekdays(Monday to
Friday, except Public Holidays)and one Saturday (14th^ January 2017) between 23 rd
December 2016 and 19th^ January 2017 (a total of 17 weekdays and 1 Saturday). In total,
1,255 eligible respondents completed the interview. The response rate was 10.8%.
Weighting was applied based on age and gender in order to make our findings more
representative, using the Hong Kong population data compiled by the Census and Statistics
Department General Household Survey Q2 2016 as reference.Associations between
selected demographic information and responsesto selected questions were examined by
the Pearson’s chi-square test, Kruskal-Wallis test and Spearman’s rank correlation.
Social Sciences Research Centre of The University of Hong Kong Page 4 of 172
Results of Survey
Knowledge of antibiotics
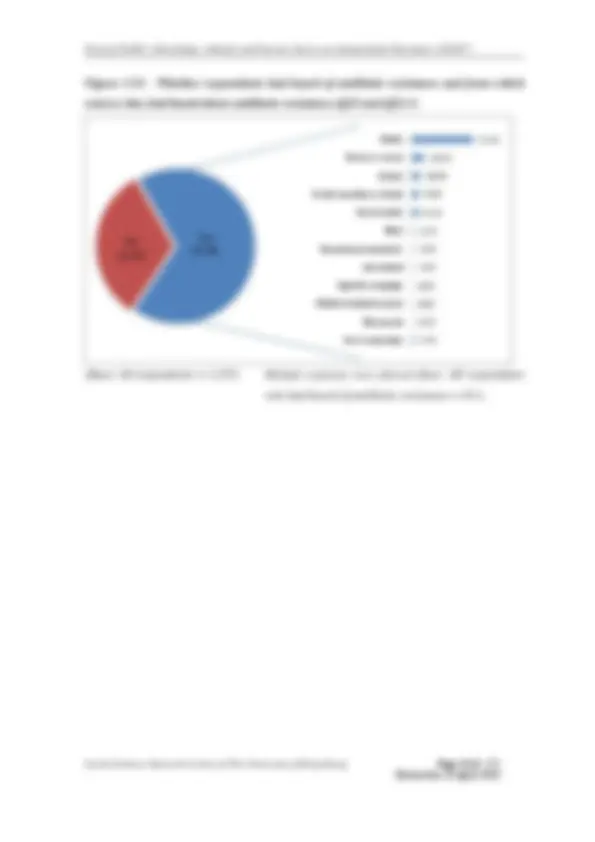
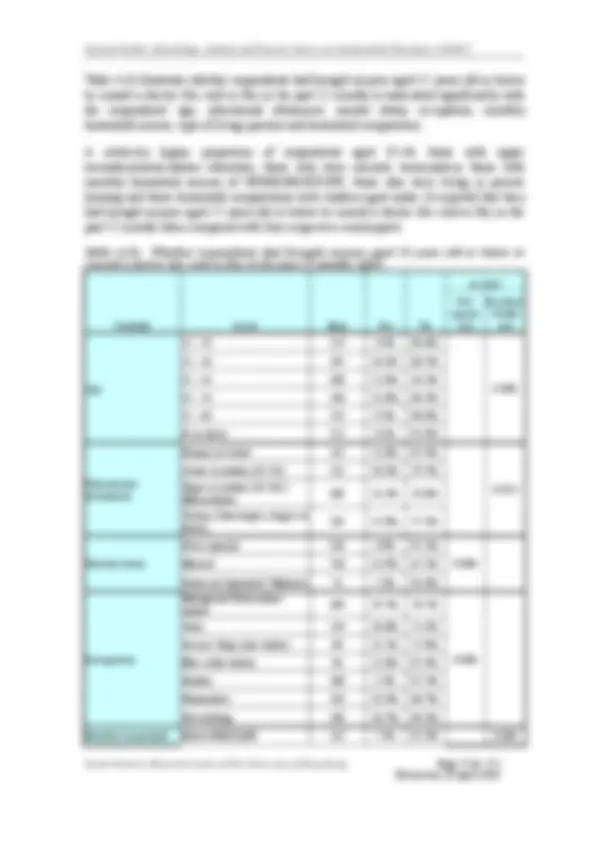
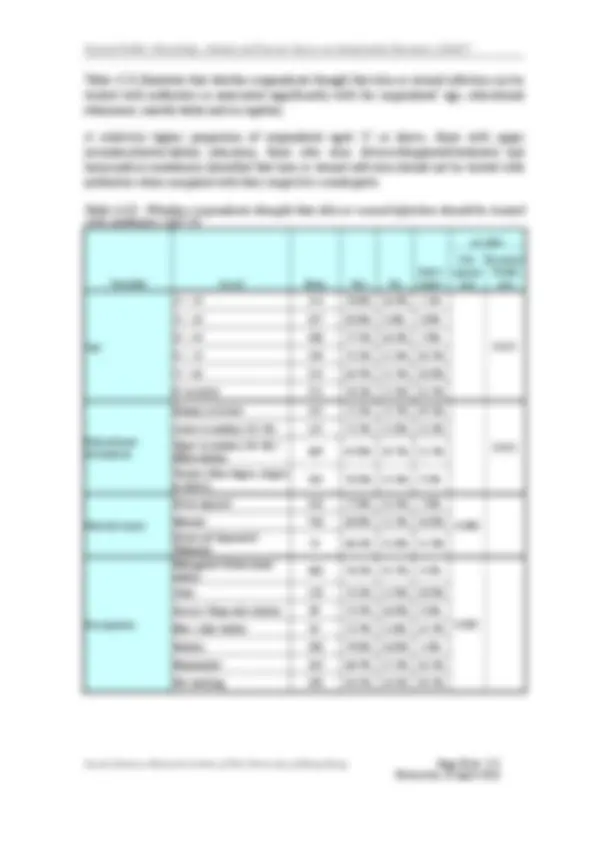
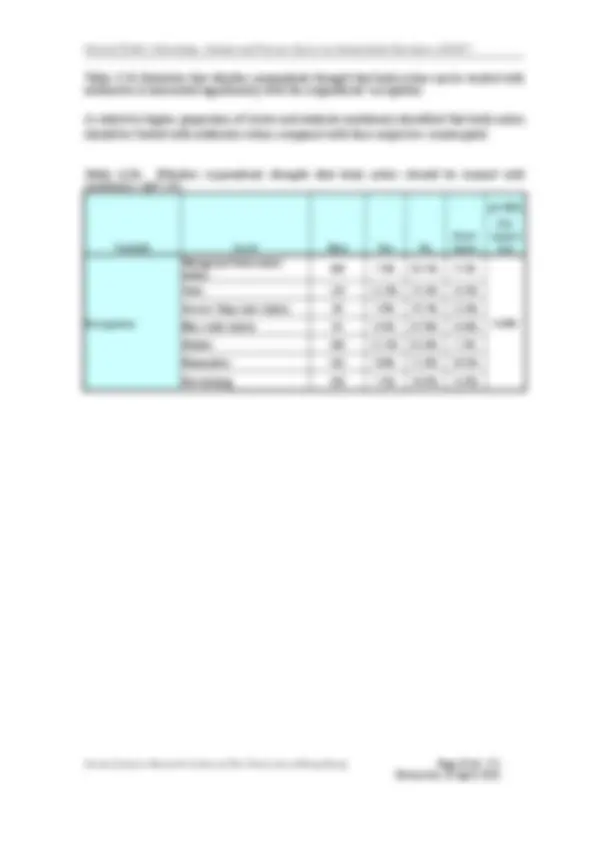
Which medical conditions should antibiotics be used to treat
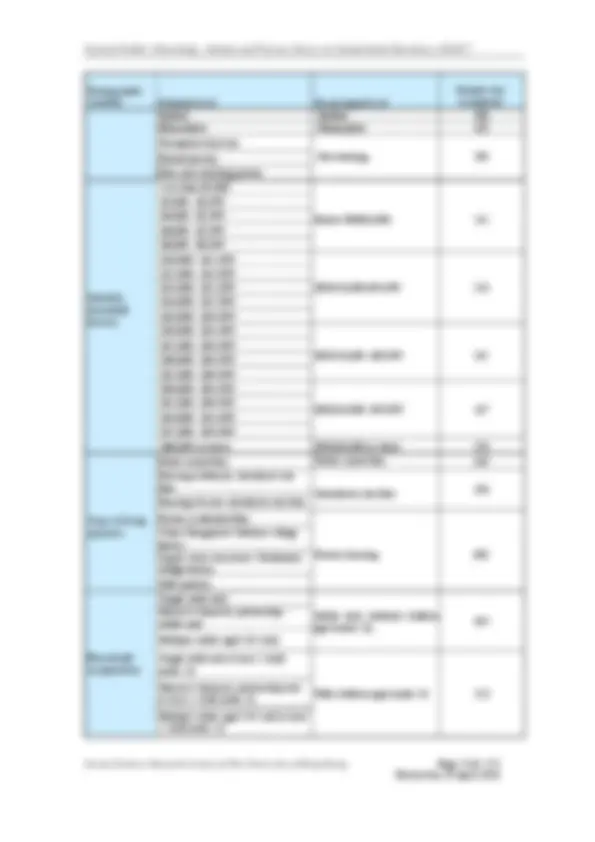
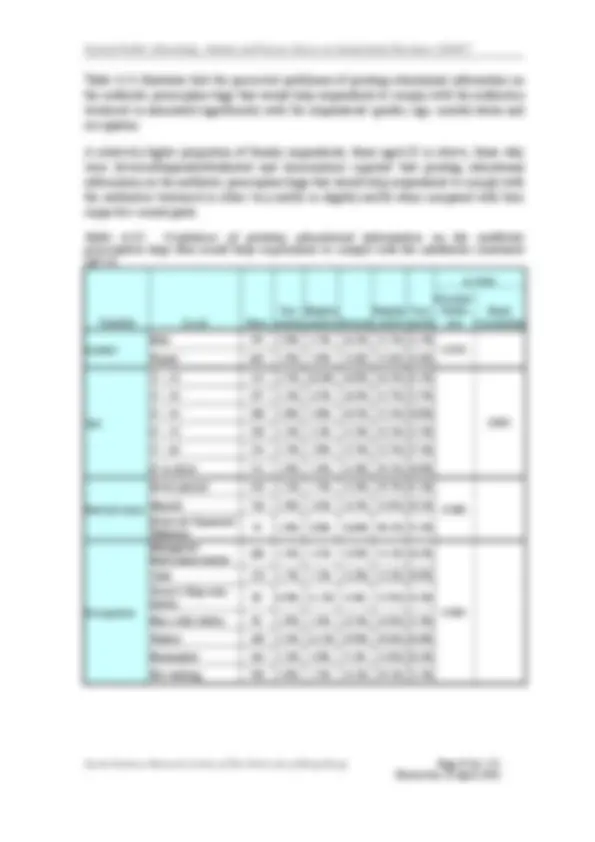
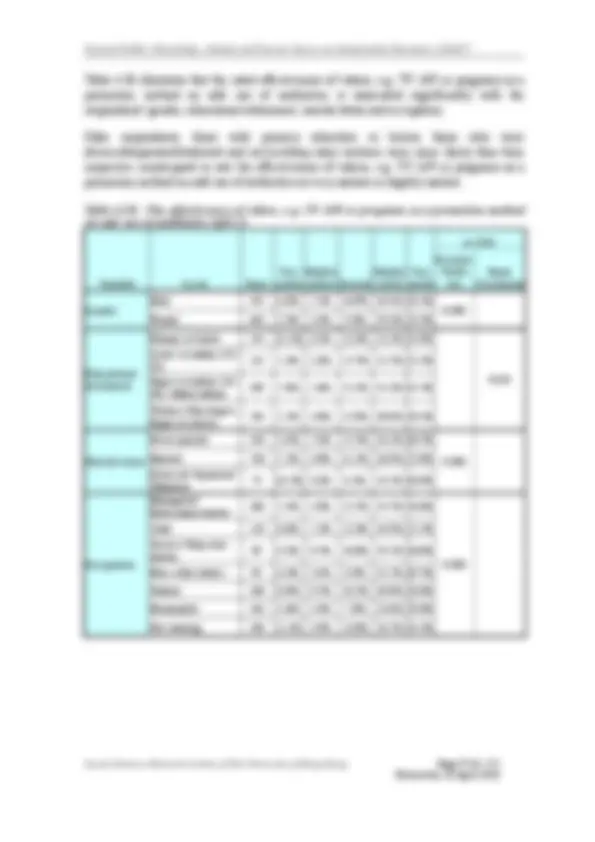
The majority of respondents correctly identified the following medical conditionsas
treatable with antibiotics:
Skin or wound infection (Can be treated: 71.8% vs Cannot be treated: 15.3%)
Bladder/urinary tract infection (UTI) (69.1% vs 13.7%)
In contrast, only 26.5% correctly identified gonorrhoea as a condition treatable with
antibiotics.
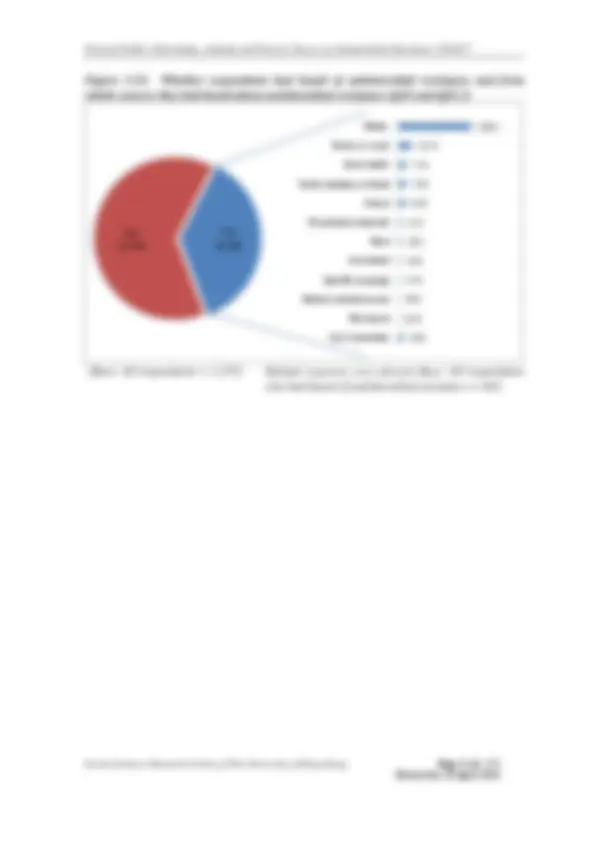
Over half of all respondents mistakenly identified the following medicalonditions c
treatable with antibiotics:
Cold and flu (54.0% vs 37.3%)
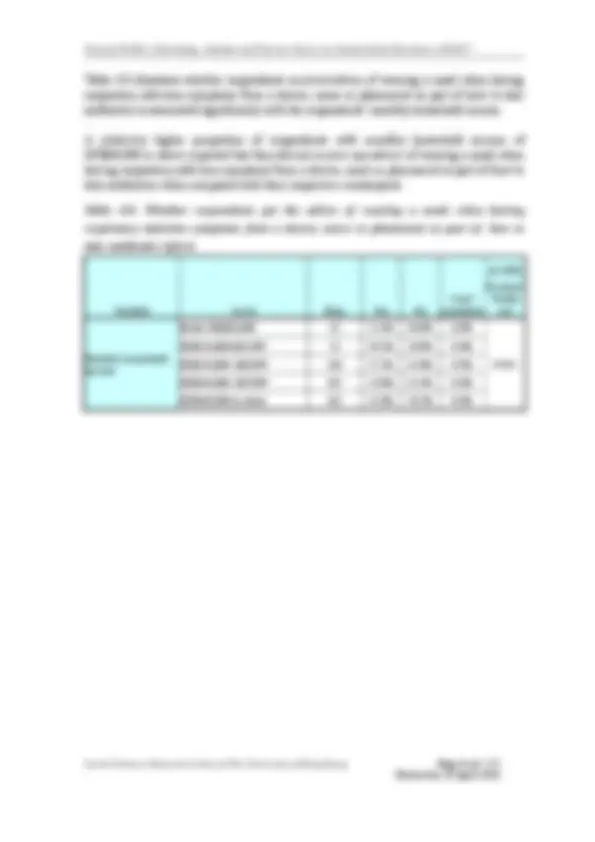
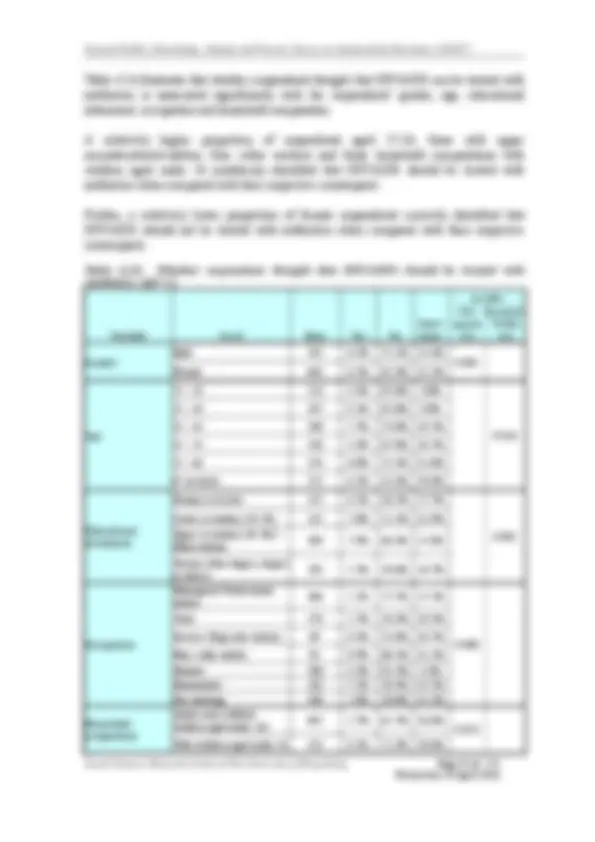
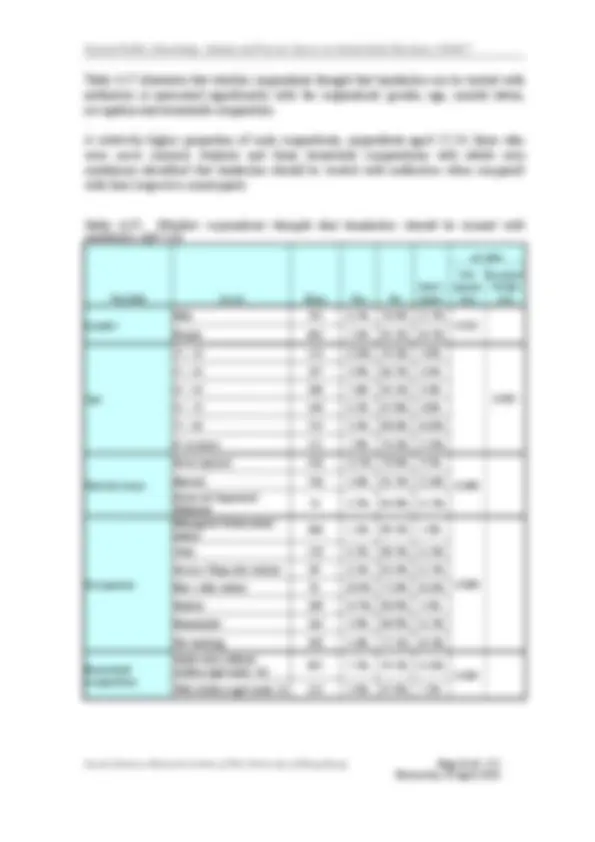
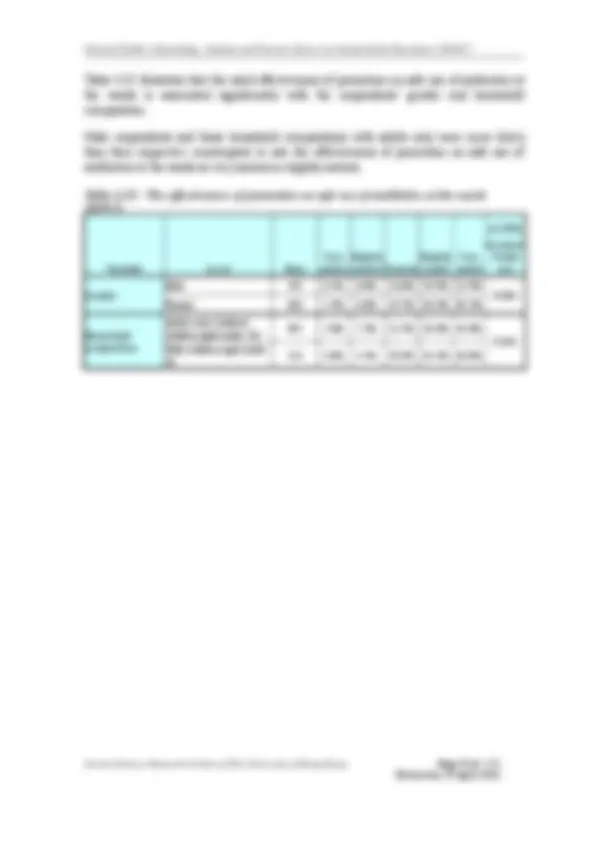
The majority of all respondents (87.9%) thoughtthey should stop taking antibioticsonly
when they have taken all of the antibiotics as directed, while one-tenth of them (10.4%)
thought they should stop taking antibiotics when they felt better and the rest (1.7%) did not
know.
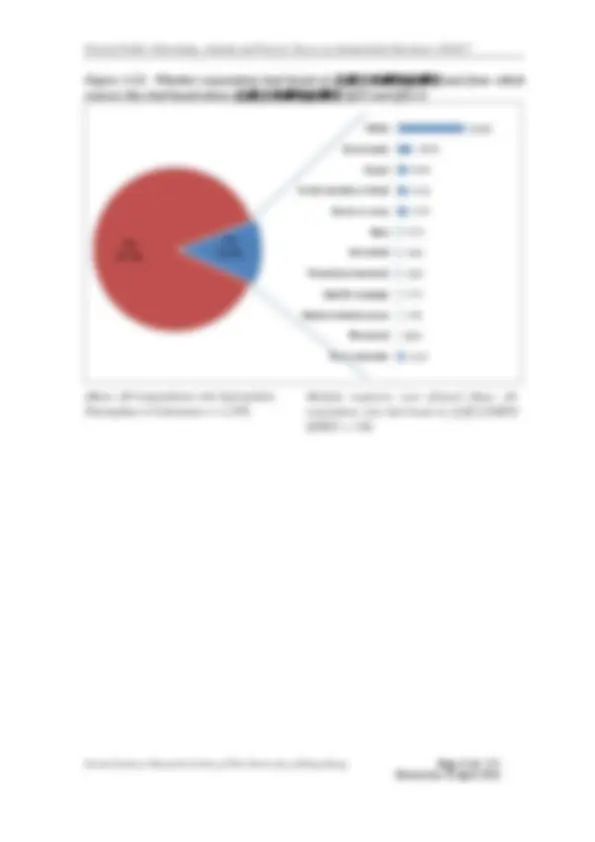
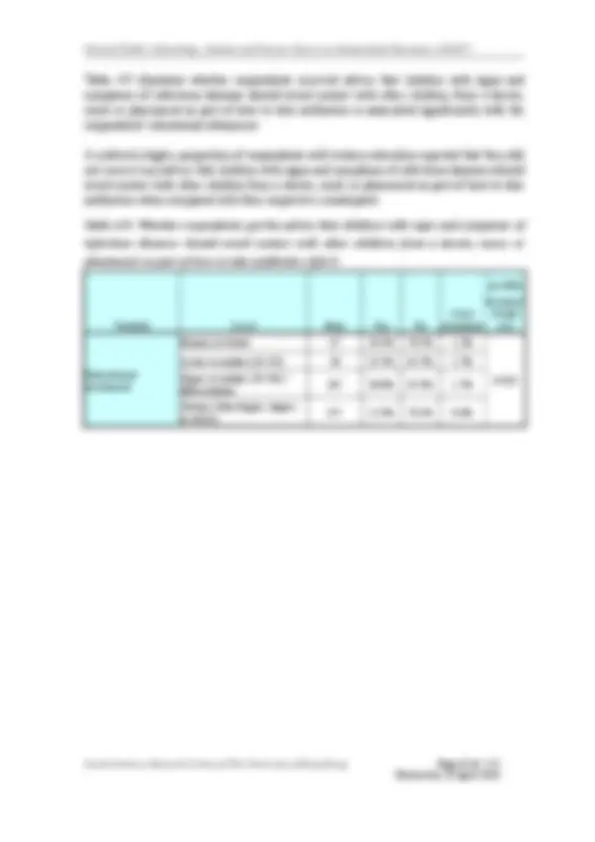
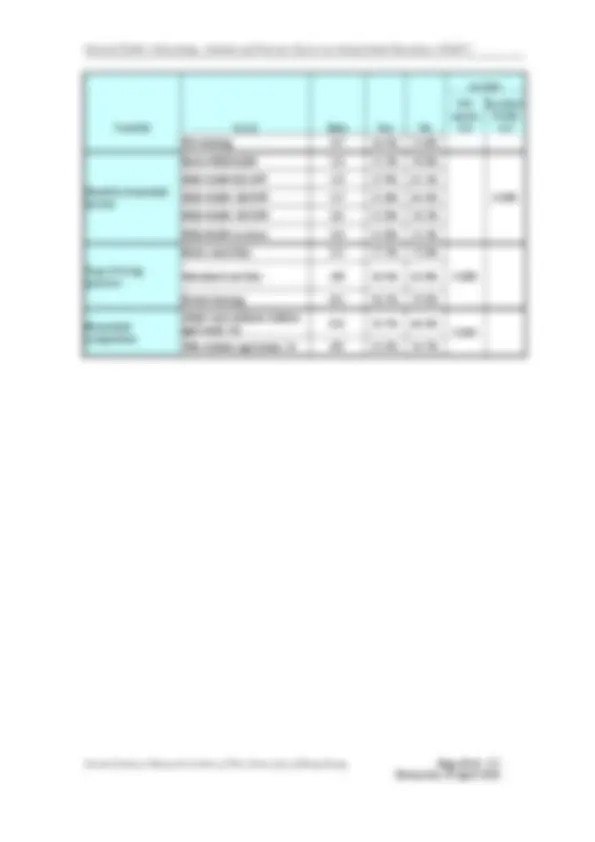
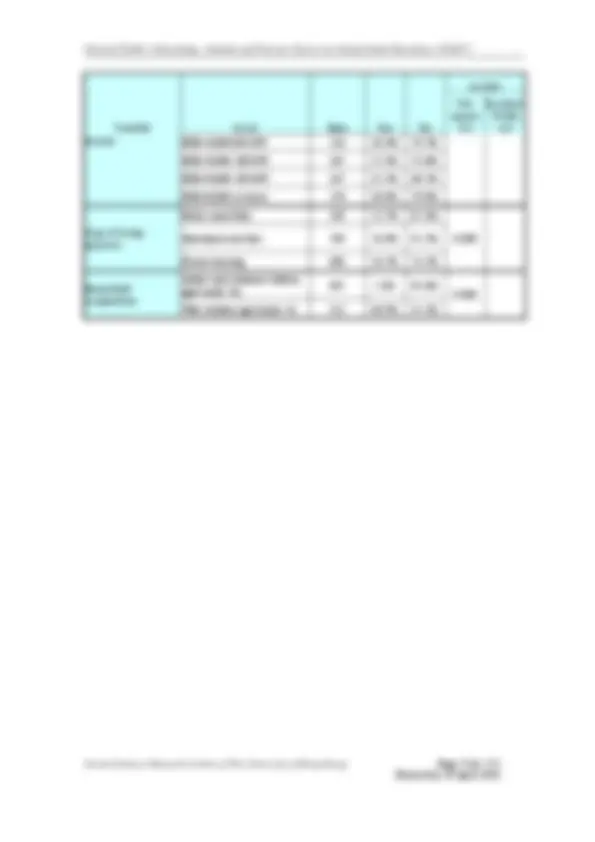
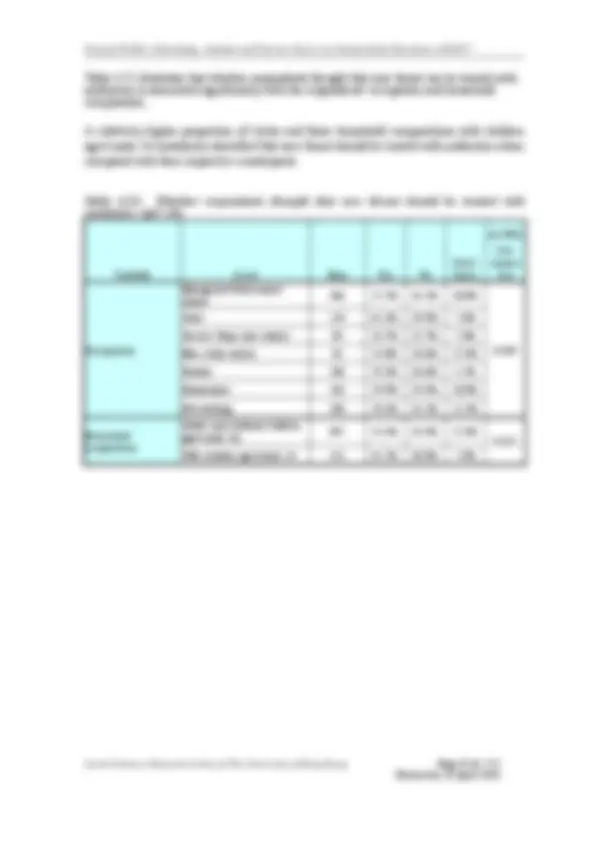
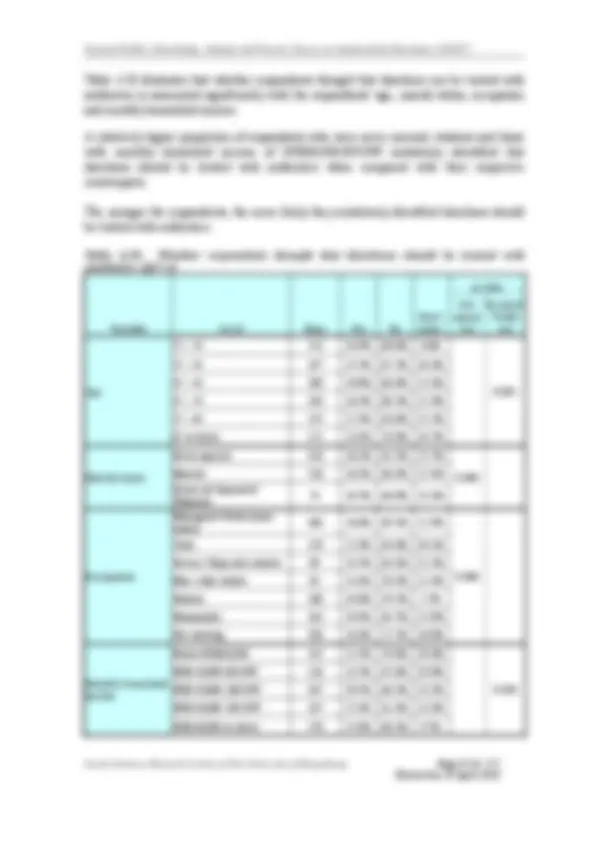
It is reassuring that the majority of all respondents correctly identified the following two
false knowledge statements about antibiotics as incorrect:
It's okay to use antibiotics that were given to a friend or family member, as long as
they were used to treat the same illness (False: 93.1% vs True: 5.9%)
It’s okay to buy the same antibiotics, or request them from a doctor, if you're sick and
they helped you get better when you had the same symptoms before (False: 83.1% vs True: 13.6%)
Social Sciences Research Centre of The University of Hong Kong Page 6 of 172
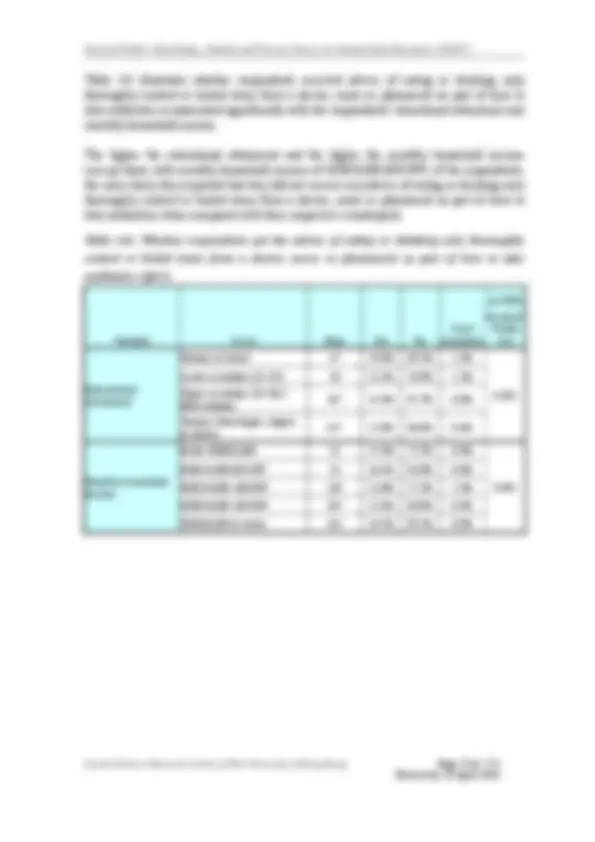
Doctors give related advice when prescribing antibiotics (76.9% vs 4.3%) Pharmacists give related advice when dispensing antibiotics (70.9% vs 7.3%)
Practices and attitude towards antibiotic use
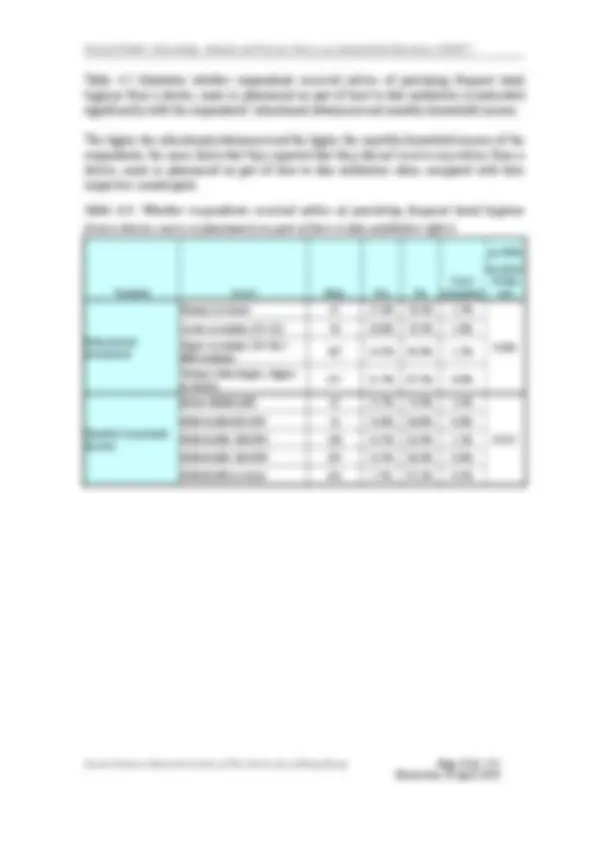
About one-third of all respondents (36.3%) reported that they preferred to consult a doctor
that has declared to use antibiotics responsibly.
Among those respondents (59.7%) who reported that they had consulted a doctor (for cold
or flu) in the past 12 months, only a very small proportion of them (2.5%, 19 respondents)
had asked for antibiotics during that consultation.
Among those respondents (21.4%) who reported that they had broughtsomeone aged 15 years old or below to consult a doctor (for cold or flu) in the past 12 months, only 2 respondents (0.9%) had asked for antibiotics for that person during that consultation.
When a doctor‘s initial assessment indicated that antibiotics are not needed, the vast majority of respondents (96.9%) would acceptthe doctor’s advice to observe for a few more days or to wait for the diagnostic test result before deciding whether to prescribe antibiotics or not.
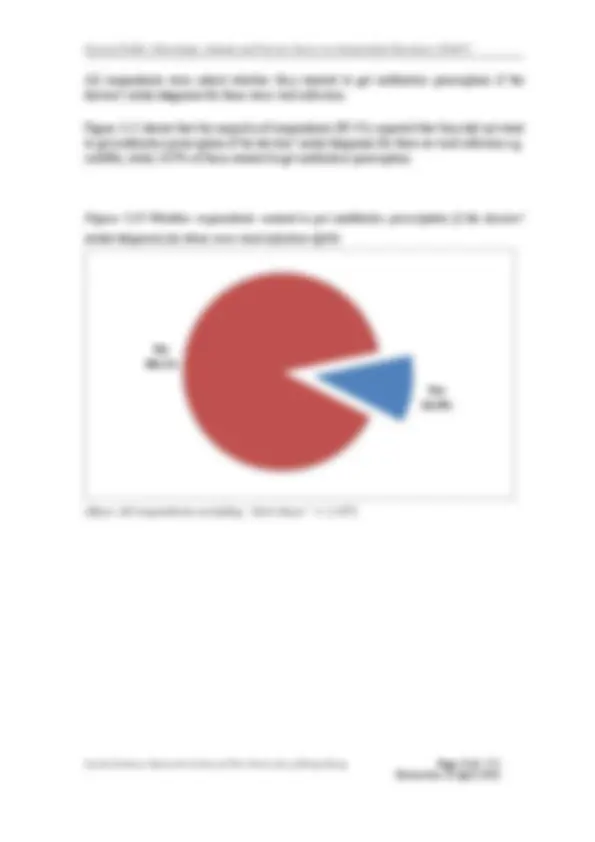
The majority of respondents (84.3%) did not want to receive any antibiotics prescription if
the doctors’ initial diagnosis for them is viral infection e.g. cold/flu, while 10.3% of them
wanted to get an antibiotics prescription.
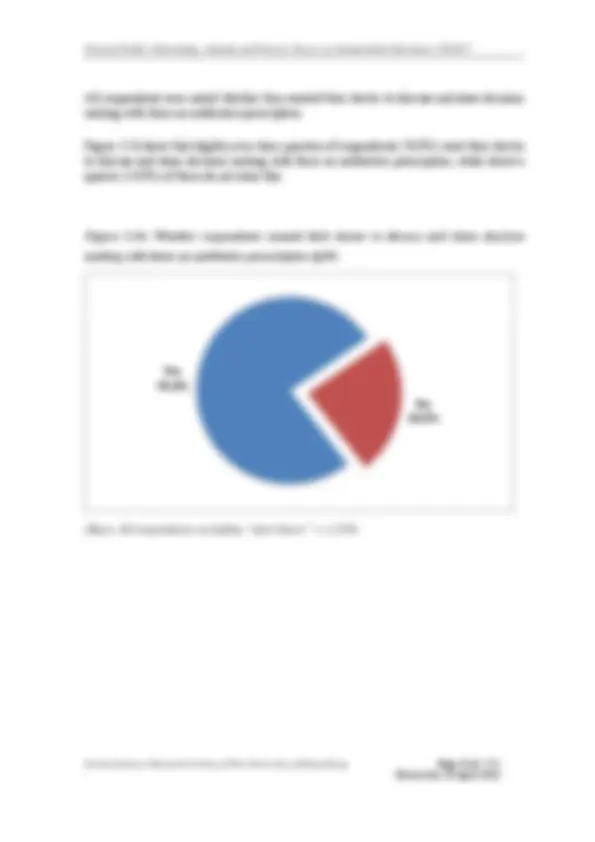
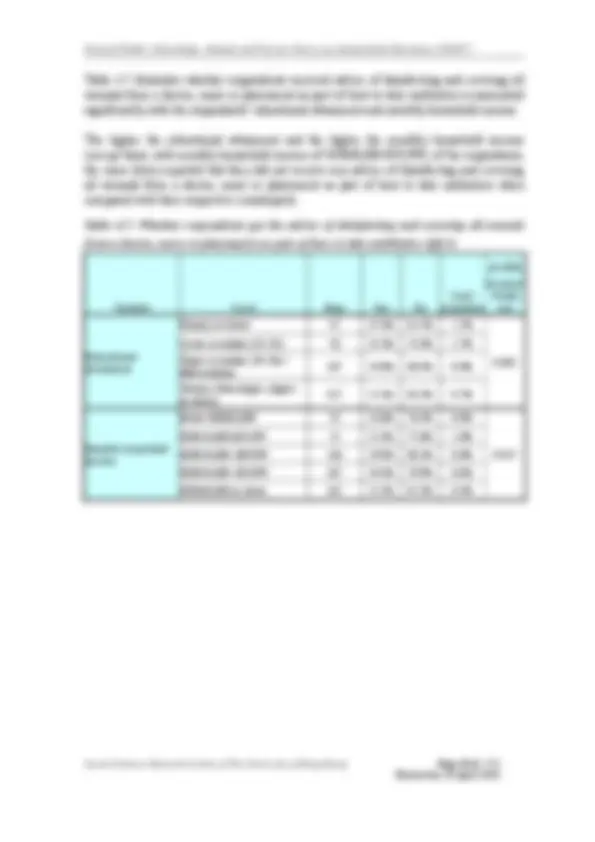
The majority of respondents (73.9%) wanted their doctor to discuss andmake a shared
decision with them on antibiotics prescription.
The effectiveness of promotion on safe use of antibiotics at a list of places
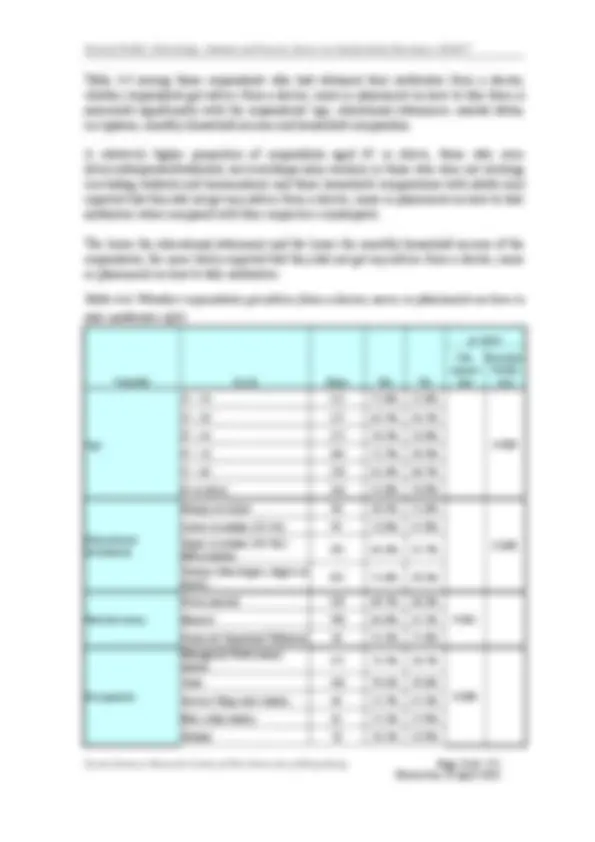
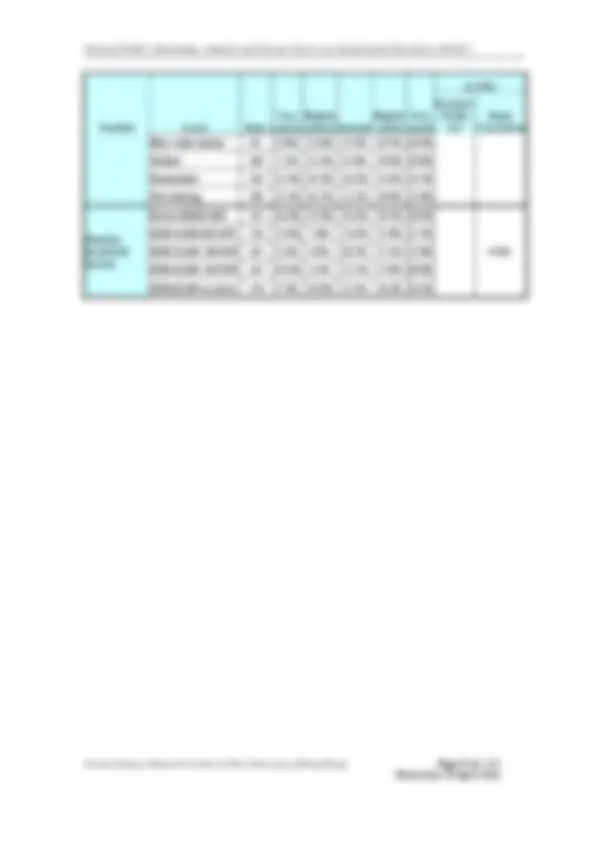
A large proportion of all respondents rated the effectiveness of promotion on safe use of
antibiotics at the following places as either very useful or slightly useful:
Hospital or Clinic pharmacies (while waiting for drug dispensing) (very useful or slightly useful: 75.6% vs very useless or slightly useless: 8.8%) Waiting areas of clinics or A&E departments (70.4% vs 12.9%) Wards (65.4% vs 13.1%) Community pharmacies (51.9% vs 23.0%)
Social Sciences Research Centre of The University of Hong Kong Page 7 of 172
The effectiveness of different media for promotion of safe use of antibiotics
A large proportion of all respondents rated the effectiveness of the following promotion methods on safe use for antibiotics as very useful or slightly useful:
Videos (e.g. TV API or programs) (very useful or slightly useful: 77.3% vs very useless or slightly useless: 9.5%) Websites or social medias, e.g. Facebook (57.9% vs 19.8%) Printed materials, e.g. posters or pamphlets (48.3% vs 22.5%) Articles, e.g. columns in newspapers or magazines (46.2% vs 23.1%)
Knowledge of antimicrobial resistance
Awareness of the terms commonly used in relation to the issue of antimicrobial
resistance
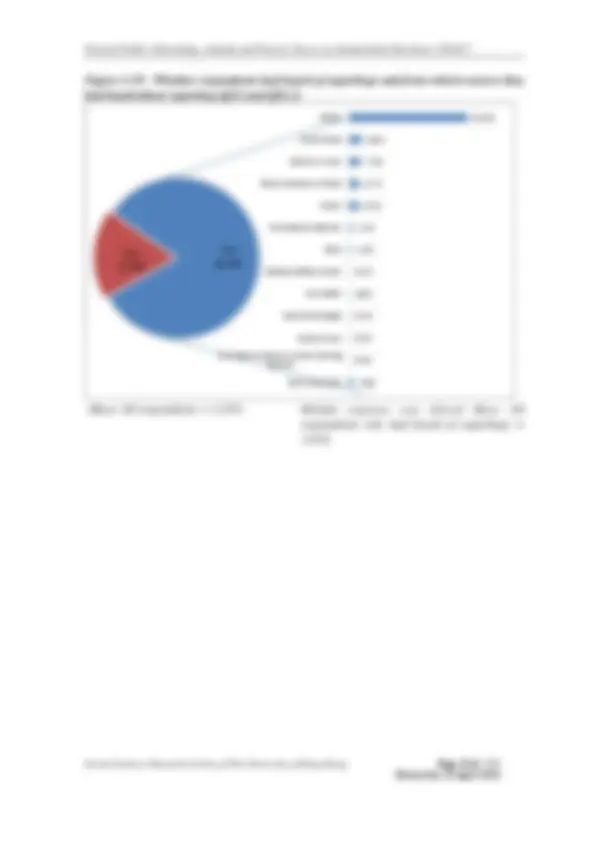
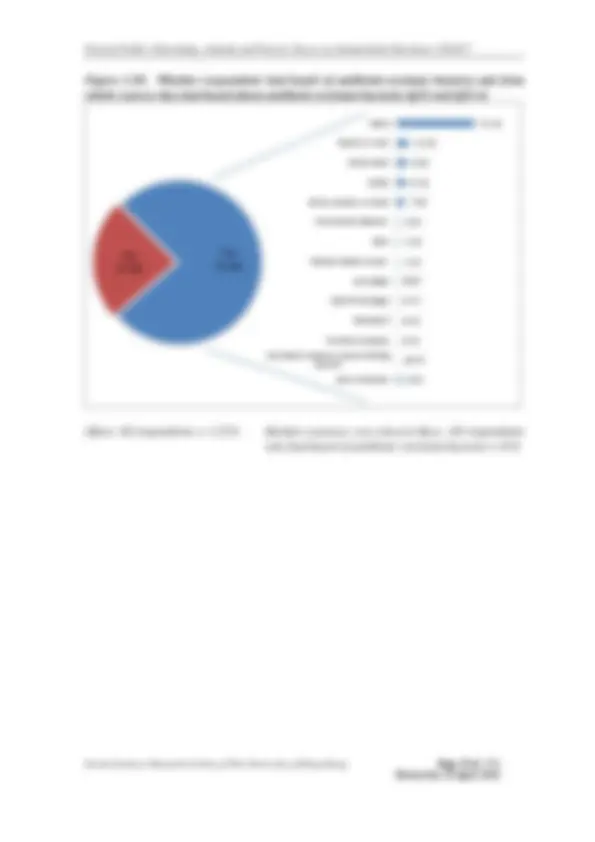
A large proportion of respondents have heard of the Chinese term of superbugs (超級細菌) (82.2%), antibiotic-resistant bacteria (抗藥性細菌)(76.2%) or antibiotic resistance (抗生 素耐藥性) (67.8%). However, only a minority of respondents have heard of antimicrobial resistance (抗菌素耐藥性) (36.8%) or 抗微生物藥物耐藥性 (12.6%, in Chinese only for those respondents who speak Putonghua or Cantonese). The media was the most common source from which they had heard about these terms.
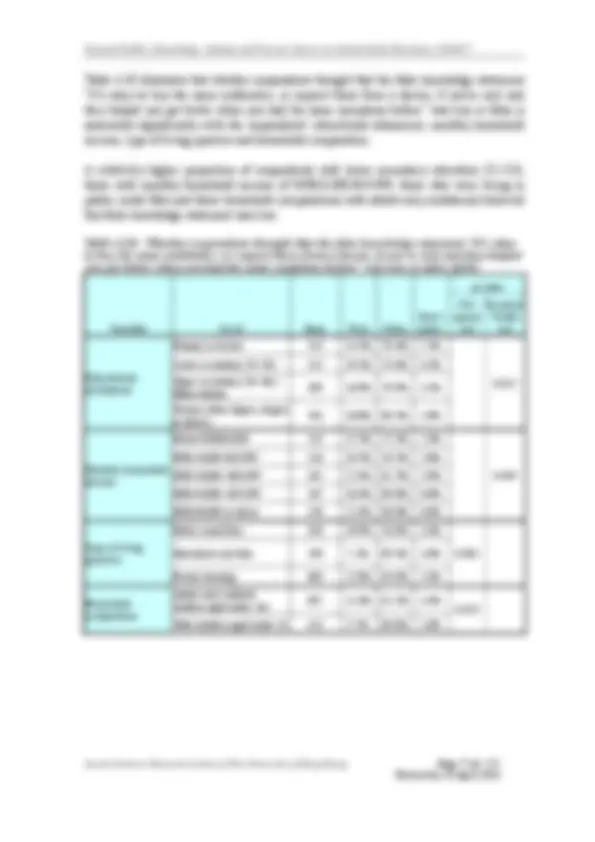
Levels of understanding of the issue of antimicrobial resistance
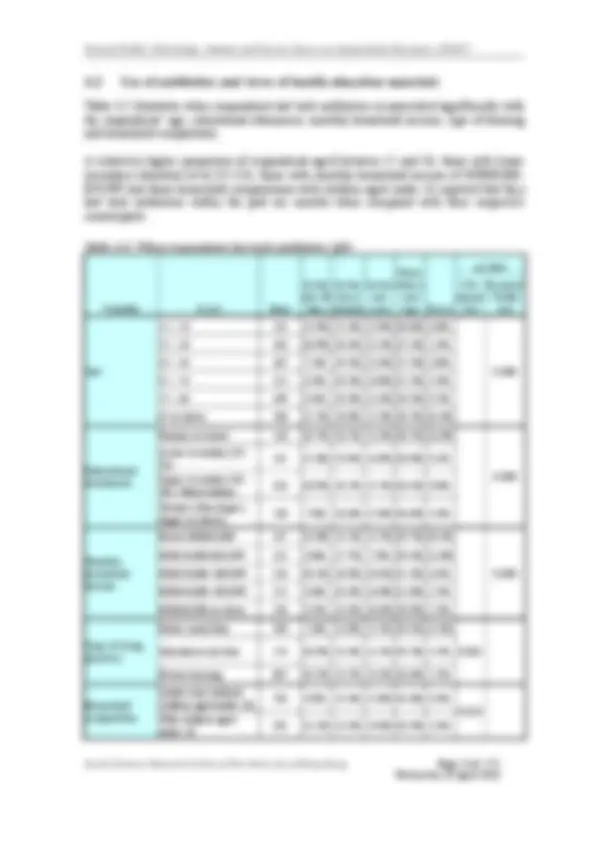
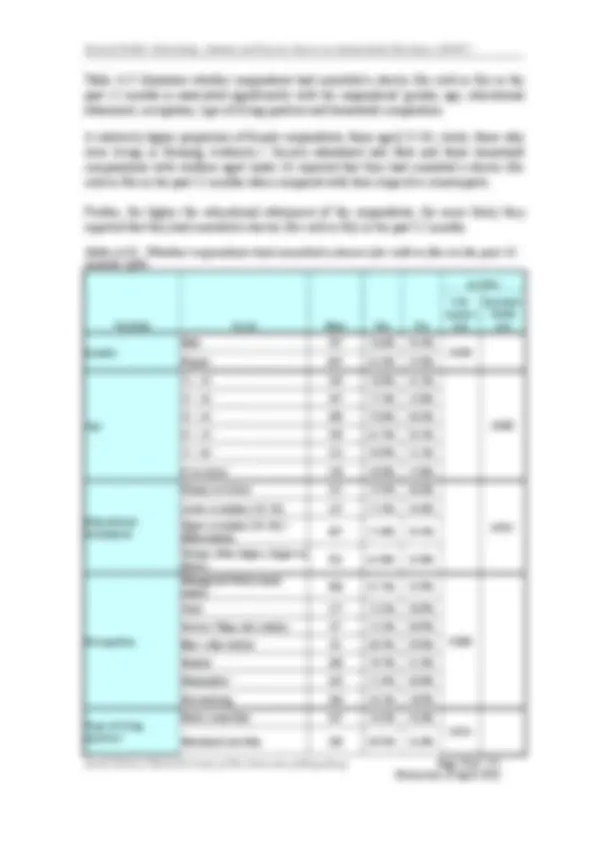
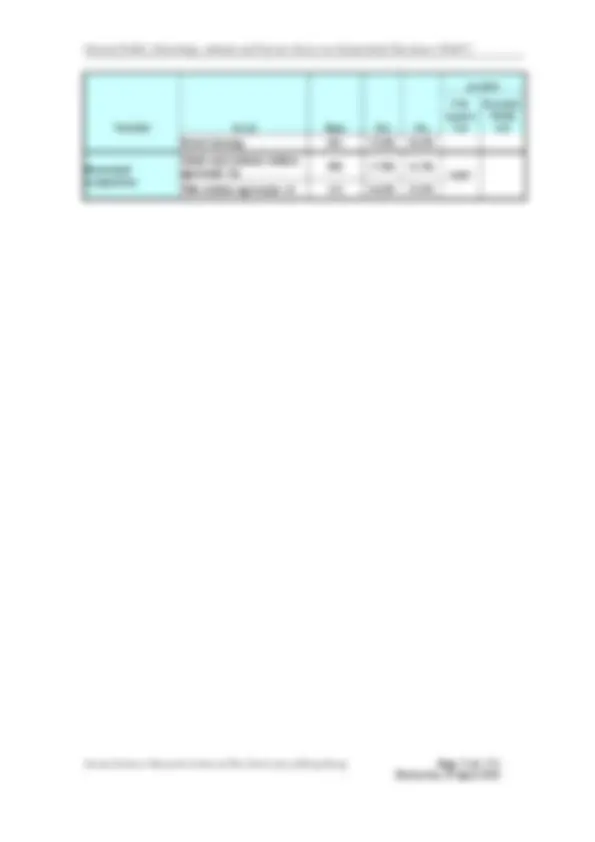
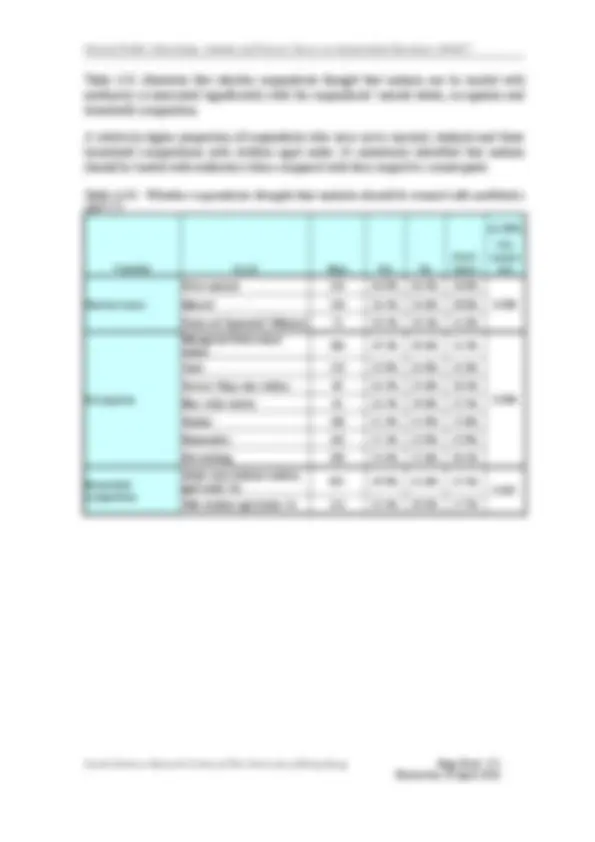
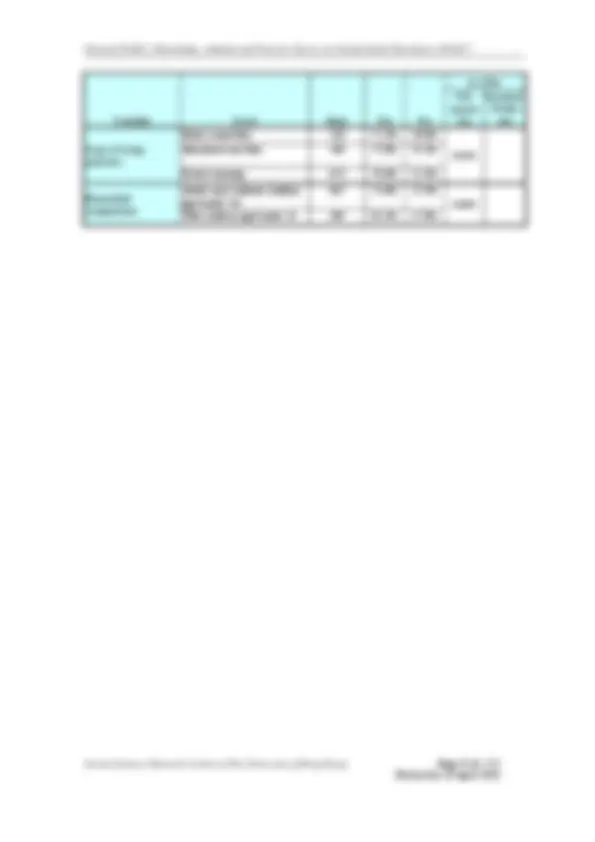
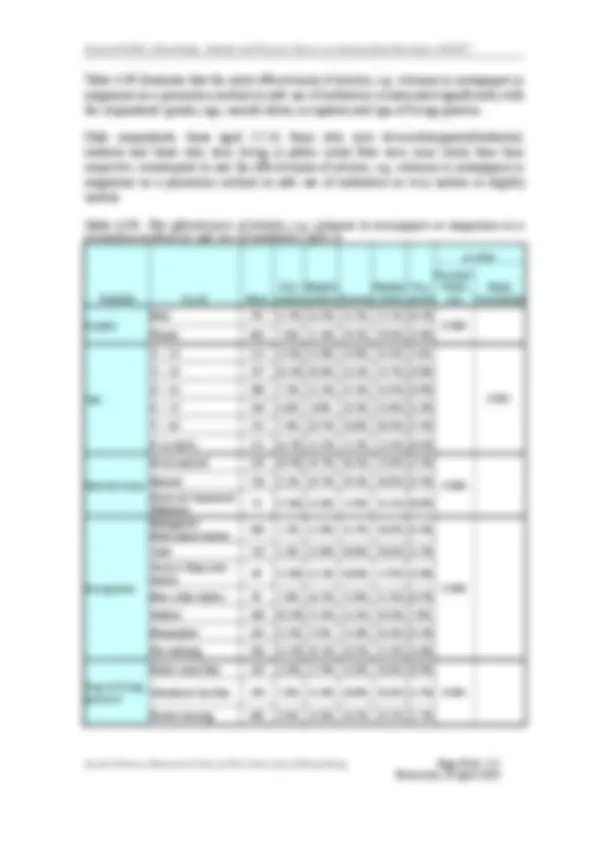
A large proportion of respondents correctly identified the following true statements:
Many infections are becoming increasingly resistant to treatment by antibiotics (True: 79.9% vs False: 8.4%) If bacteria are resistant to antibiotics, it can be very difficult or impossible to treat the infections they cause (73.8% vs 15.9%) Antibiotic-resistant infections could make medical procedures like surgery, organ transplants and cancer treatment much more dangerous (72.3% vs 11.6%) Antibiotic resistance is an issue that could affect me or my family (68.6% vs 18.3%)
One third of respondents misunderstood that bacteria which are resistant to antibiotics cannot be spread from person to person (36.9%)
A large proportion of respondents (76.5%) mistakenly identified “Antibiotic resistance occurs when your body becomes resistant to antibiotics and they no longer work as well” was a true statement. Nonetheless,the majority of them recognised “Antibiotic resistance is an issue in other countries but not here” (81.8%)and “Antibiotic resistance is only a problem for people who take antibiotics regularly” (53.2%) were false statements.
Social Sciences Research Centre of The University of Hong Kong Page 9 of 172
Recommendations
This study showed that the majority of respondents were aware ofantibiotic resistance and
its risk, although not familiar with the Chinese terminology of antimicrobial resistance (抗
菌素耐藥性) and 抗微生物藥物耐藥性. However, half of them considered themselves
incapable of stopping the AMR problem. This study also identified that misunderstanding
on indications of antibiotics remain prevalent with over half of the respondents mistaking
cold and flu as conditions treatable with antibiotics. Awareness-raising activities of the
general public should be strengthened to fill this knowledge gap in future health promotion
programmes. It is noteworthy that most respondents would comply with doctor’s advice on
the need of antibiotics for cold and flu or viral infections. Therefore, health advice and
education provided during medical consultations can also serve as a powerful intervention
in reducing inappropriate antibiotic use.
Most respondents showed support to potential AMR control measures, including shared
decision-making on antibiotic prescription, and most accepted “noantibiotic prescription
with watchful-waiting” when the initial medical assessment indicated antibiotics is not
needed. To carry this forward, guidelines and training for primary care providers and
patient materials can facilitate shared decision-making and “no antibiotic prescription with
watchful waiting” practice in community setting. More studies should also be conducted to
further assess the needs of prescribers and how the above interventions can be facilitated.
Finally, traditional mode of message delivery by (TVvideos API or television
programmes), website or social media were considered useful by most respondents. Future
health promotion should also explore and expand channels of delivery in waiting area of
hospital, pharmacies clinics and emergency departments which were considered effective
for delivery of health message on proper antibiotic use.
It would be helpful to repeat a similar KAP survey in order to monitor trend in local
population, assess the effectiveness of interventions and guide future actions.
Social Sciences Research Centre of The University of Hong Kong Page 10 of 172
Chapter One Introduction
The Social Science Research Centre of The University of Hong Kong (“HKUSSRC”) was commissioned by the Department of Health (“DH”) to conduct a territory-wide telephone survey in December 2016. This survey was designed to measure the knowledge, attitude and practice (“KAP”) ofthe general public on antibiotics and their awareness of Antimicrobial Resistance (“AMR”).
The objectives of the survey are:
A. To collect information on KAP ofthe general public regarding antibiotic use and AMR including:
a. General public understanding on the effect of antibiotics;
b. General public attitude and practice on antibiotic use; and
c. General public awareness of antimicrobial resistance problem.
B. To explore the general public views on potential measures against AMR
On the weekdays, telephone calls were made between 4:00 p.m. and 10:30 p.m. On the Saturday, telephone calls were made between 1:00 p.m. and 6:00 p.m.
2.6 Response rate
A total of 22,966 telephone numbers were attempted. The number of fully enumerated cases was 1,255 while there were 168 partially enumerated cases and 392 refusal cases. 6,242 cases were classified as non-contact cases in which eligible persons were not-at- home or not available. An unanswered telephone call had been tried at least5 contact attempts before classifying as non-contact case, including one contact attempt in day time to eliminate the business telephone numbers in non-contact cases. The contact rate was 40.0% 2 and the overall response rate was 10.8%^3. Table 2.1 shows the detailed breakdown of final telephone contact status.
Table 2.1: Final status of telephone numbers attempted
Final status of contacts^4 Number of cases (A) No. of telephone numbers sampled 22,
(B) No. of ineligible cases 10,
a) Valid working telephone numbers 1, i) Claimed wrong number 0 ii) Language problem 32 iii) Non-residential line 1, iv) No target respondent 51 b) Invalid telephone numbers 9, i) Fax / data line 945 ii) Non-working / out of service number 8,
(C) No. of eligible cases 8,
a) Successfully completed interviews 1, b) Unsuccessful cases 6, i) Mid-way termination cases 168
(^2) Contact rate = the number of answered telephone calls divided by the total number of calls attempted, i.e.
from Table 2.6, Sum of ((B)(a)(ii), (B)(a)(iii), (B)(a)(iv), (C)(a), (C)(b)(i), (C)(b)(ii) and (C)(b)(iii)) / Total = (32+1,042+51+1,255+168+6,242+392) / 22,966 = 40.0%. 3 Response rate = the number of completed interviews divided by the estimated total number of eligible cases, i.e. from Table 2.6, C(a) * (1 / (C + D * C / (B(a) + C))) * 100% = 1,255 * (1 / (8,057+4,052*8,057/ (1,125+8,057))) * 100% =10.8%. 4 “Language problem”: eligible respondents who were not able to speak clearly in any of the specified languages such as Cantonese, Putonghua or English. “Non-working / out of service number”: not a valid telephone line (because we used a random method to generate telephone numbers, see section 2.1). “Mid-way termination”: eligible respondents who initially accepted the interview but failed to complete the interview due to some reasons. “Not available”: eligible respondents who were busy at the timeof telephone contact. “Refusal cases”: eligible respondents who refused the interview. Social Sciences Research Centre of The University of Hong Kong Page 12 of 172
Social Sciences Research Centre of The University of Hong Kong Page 13 of 172
Final status of contacts^4 Number of cases ii) Non-contact cases such as selected eligible person not-at- home / not available 6, iii) Refusal cases 392
(D) No. of cases with unknown eligibility status^5 4, a) Answering machine 0 b) Busy line 0 c) Call blocking, password needed 0 d) Immediate disconnection^6 e) No answer 4,
2.7 Sample size and sampling error
A sample size of1,255 successful interviews was achieved (the target sample size was 1,070) The width of a 95% confidence interval for this sample size is at most +/− 2.8%^7. This means that we can have 95% confidence that the true population proportion falls within the sample proportion plus or minus 2.8%. For example, 36.3% of the respondents reported that they preferred to consult a doctor that has declared to use antibiotics responsibly and then the conservative 95% confidence interval for the true percentage of the population falls between 36.3% ± 2.8%, i.e. 39.1% and 33.5%.
2.8 Quality control
All HKUSSRC interviewers were well trained in a standardised approach prior to the commencement of the survey. All interviews were conducted by experienced interviewers fluent in Cantonese, Putonghua and English.
The HKUSSRC engaged in quality checks for each stage of the survey to ensure satisfactory standard of performance. At least 15% of the questionnaires completed by each interviewer were checked by the SSRC independently.
2.9 Statistical analysis and weighting
This survey revealed some differences in gender and ageproportions when compared with the Hong Kong population data compiled by the Census and Statistics Department (C&SD) General Household Survey Q2 2016. The proportions of respondents among age groups 50-54, 60-64, 65-69 and 70-74 were much higher than the population while the proportions of respondents aged 15-19, 25-29, 30-34, 35-39 and 80 years and above were much lower.
(^5) Including only those telephone numbers with unknown eligibility status in all call attempts made so far. The breakdown of (D) shows only the latest / final call disposition of these cases. 6
7 Including those cases which the calls disconnected before the cases could be classified as eligible. As the population proportion is unknown, 0.5 is put into the formula of the sampling error to produce the most conservative estimate of the sampling error. The confidence interval width is then:
± 1. 96 ×^0. 12555 ×^0.^5 × 100 %=±2.8 %
Social Sciences Research Centre of The University of Hong Kong Page 15 of 172
Sample ratio
Sample weightforthecorrespondinggenderandage = Populationratio
If respondents refused to provide their age information, the sample weight is set as 1.
Table 2.3 Weights by age and gender applied in the analyses Age Male Female 15 - 19 1.204094649 1. 20 - 24 1.278277713 0. 25 - 29 2.551031232 1. 30 - 34 2.489540970 1. 35 - 39 2.725371371 1. 40 - 44 1.178354114 0. 45 - 49 1.305053872 0. 50 - 54 1.276015699 0. 55 - 59 1.077066933 0. 60 - 64 1.084618223 0. 65 - 69 0.871936742 0. 70 - 74 0.612820761 0. 75 - 79 1.164200955 0. 80+ 1.155703138 1. Age data missing 1. 000000000 1.00000 0000
Statistical tests were applied to detect any significant differences between-groups. sub Associations between selected demographic information and responses of selected questions were also examined. Significance testing was conducted at the 5% level- ( tailed). The statistical software, IBM SPSS for Windows version 23.0 was used to perform all statistical analyses.
Social Sciences Research Centre of The University of Hong Kong Page 16 of 172
Chapter Three Findings of the Survey
This chapter presents the findings of this survey after weighting for gender and age. Some percentages in the figures may not add up to the total or 100% because of rounding.
3.1 Demographics
This section briefly describes the characteristics ofthe respondents in this survey (Table 3.1).
3.1.1 Gender and age
As gender and age were applied to compile weightings in this survey, the distribution of gender and age reported in this report matches the Hong Kong population data compiled by the C&SD General Household Survey Q2 2016 (Table 2.2).
Overall, 52.8% of the respondents were females and 51.9% were aged between 25 and 54.
3.1.2 Marital status
Over half of the respondents (59.4%) were married with child(ren) (53.9%) or without child (5.6%), while over a third (34.6%) of them were never married and were1.6% divorced or separated. The remaining 4.4% of the respondents were widowed.
3.1.3 Educational attainment
About half of the respondents (46.7%) had tertiary education, followed by upper secondary education (31.1%) and lower secondary education (10.8%). The remaining (11.4%) had primary education or below.
3.1.4 Occupation
Over half of the respondents (55.0%) were currently engaged in a job. Of these, 13.2% were clerks, 9.6% were employer/ managers/ administrators and 8.5% were professionals.
The rest (45.0%) of the respondentswere not currently engaged in a job including the retired persons (20.2%) and homemakers (13.7%).
Social Sciences Research Centre of The University of Hong Kong Page 18 of 172
Table 3.1: Demographic information (Continued) Educational attainment Base = 1,251 Type of Housing Base =1, Primary or below 11.4% Public rental flats 27.8% Lower secondary (S1- S3) 10.8%^
Housing Authority subsidized sale flat 12.9% Upper secondary (S4- S6)/Matriculation 31.1%^
Housing Society subsidized sale flat 2.7% Tertiary (Non-degree, degree or above) 46.7%^ Private residential flats^ 51.3%
Household composition Base =1,208 Villas/Bungalows/Modern village houses 2.5%
Single adult only 7.8%
Simple stone structures/Traditional village houses
1.4%
Single adult and at least 1 child under 16 0.2%^ Staff Quarters^ 1.3% Married / domestic partnership - adults only 12.1%^ Non-domestic quarters^ 0.1% Married / domestic partnership and at least 1 child under 16
14.1%
Multiple adults aged 16+ only 54.2% Multiple adults aged 16+ and at least 1 child under 16
11.6%
Monthly Personal Income Base = 1,159^ Monthly Household Income^ Base = Below $ 10,000 48.2% Below $ 10,000 14.0% $10,000-$19,999 17.8% $10,000-$19,999 13.4% $20,000-$29,999 12.8% $20,000-$39,999 28.2% $30,000-$49,999 10.6% $ 40 ,000-$59,999 17. 7 % $50,000 or above 10.6% $60,000 or above 26.6%
Social Sciences Research Centre of The University of Hong Kong Page 19 of 172
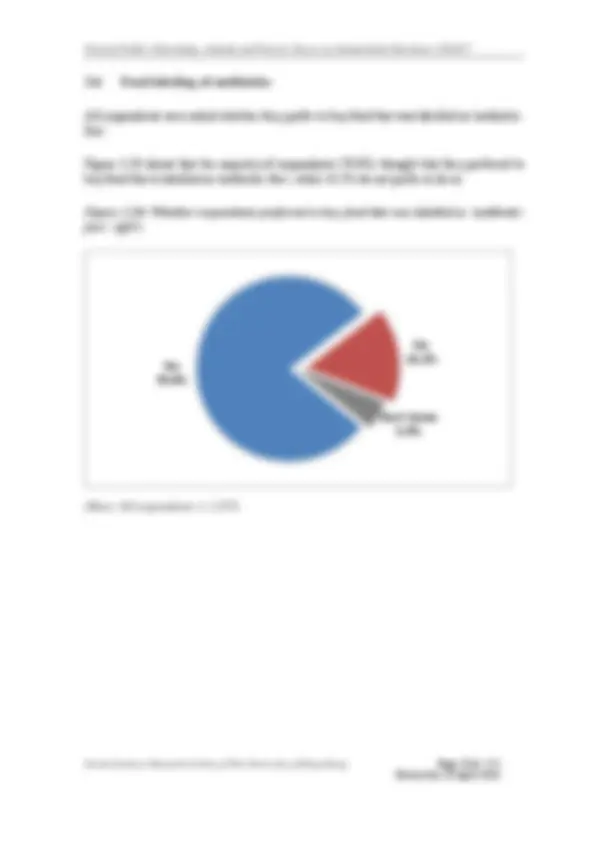
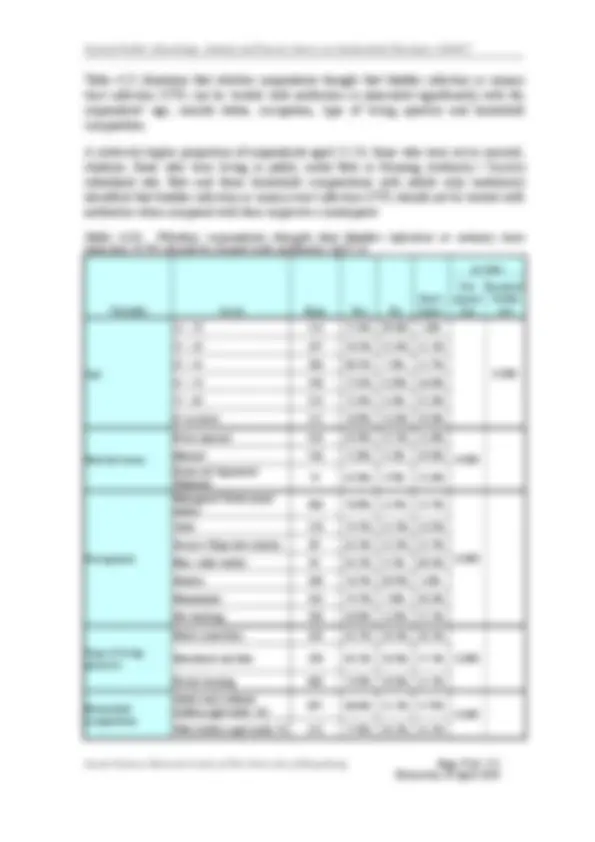
3.2 Use of antibiotics and views of health education materials
This section presents when respondents last took antibiotics, and how and where they obtained them.
Figure 3.1 shows that a third of the respondents (33.0%) reported that they last took antibiotics within the past six months, while 15.1% reported that they last took antibiotics within the past seven to twelve months.
Figure 3.1: When respondents last took antibiotics (Q1)
(Base: All respondents excluding ”can’t remember” = 1,107)
Never
More than a year ago
In the last year
In the last 6 months
In the last 30 days