


Wound Repair
Part 4













Prepara tus exámenes y mejora tus resultados gracias a la gran cantidad de recursos disponibles en Docsity

Gana puntos ayudando a otros estudiantes o consíguelos activando un Plan Premium

Prepara tus exámenes
Prepara tus exámenes y mejora tus resultados gracias a la gran cantidad de recursos disponibles en Docsity
Prepara tus exámenes con los documentos que comparten otros estudiantes como tú en Docsity
Encuentra los documentos específicos para los exámenes de tu universidad
Estudia con lecciones y exámenes resueltos basados en los programas académicos de las mejores universidades
Responde a preguntas de exámenes reales y pon a prueba tu preparación
Consigue puntos base para descargar
Gana puntos ayudando a otros estudiantes o consíguelos activando un Plan Premium
Comunidad
Pide ayuda a la comunidad y resuelve tus dudas de estudio
Ebooks gratuitos
Descarga nuestras guías gratuitas sobre técnicas de estudio, métodos para controlar la ansiedad y consejos para la tesis preparadas por los tutores de Docsity
CIRUGIA DENTAL DEL CAPITULO 4!!
Tipo: Resúmenes
1 / 42

Esta página no es visible en la vista previa
¡No te pierdas las partes importantes!
An important aspect of any surgical procedure is the preparation of the wound for proper healing. Tissue injury can be caused by pathologic conditions or by traumatic events. The dental surgeon has some control over pathologic tissue damage such as the likelihood of a wound infection.
Wound Repair
Wound Repair
Epithelialization Once the wound is fully epithelialized, the scab loosens and eventually dislodges The process of reepithelialization (i.e., secondary epithelialization) is sometimes used therapeutically by oral-maxillofacial surgeons during certain preprosthetic surgical procedures in which an area of oral mucosa is denuded of epithelium (i.e., unattached gingiva) and then left to epithelialize by adjacent epithelium (i.e., attached gingiva) creeping over the wound bed.
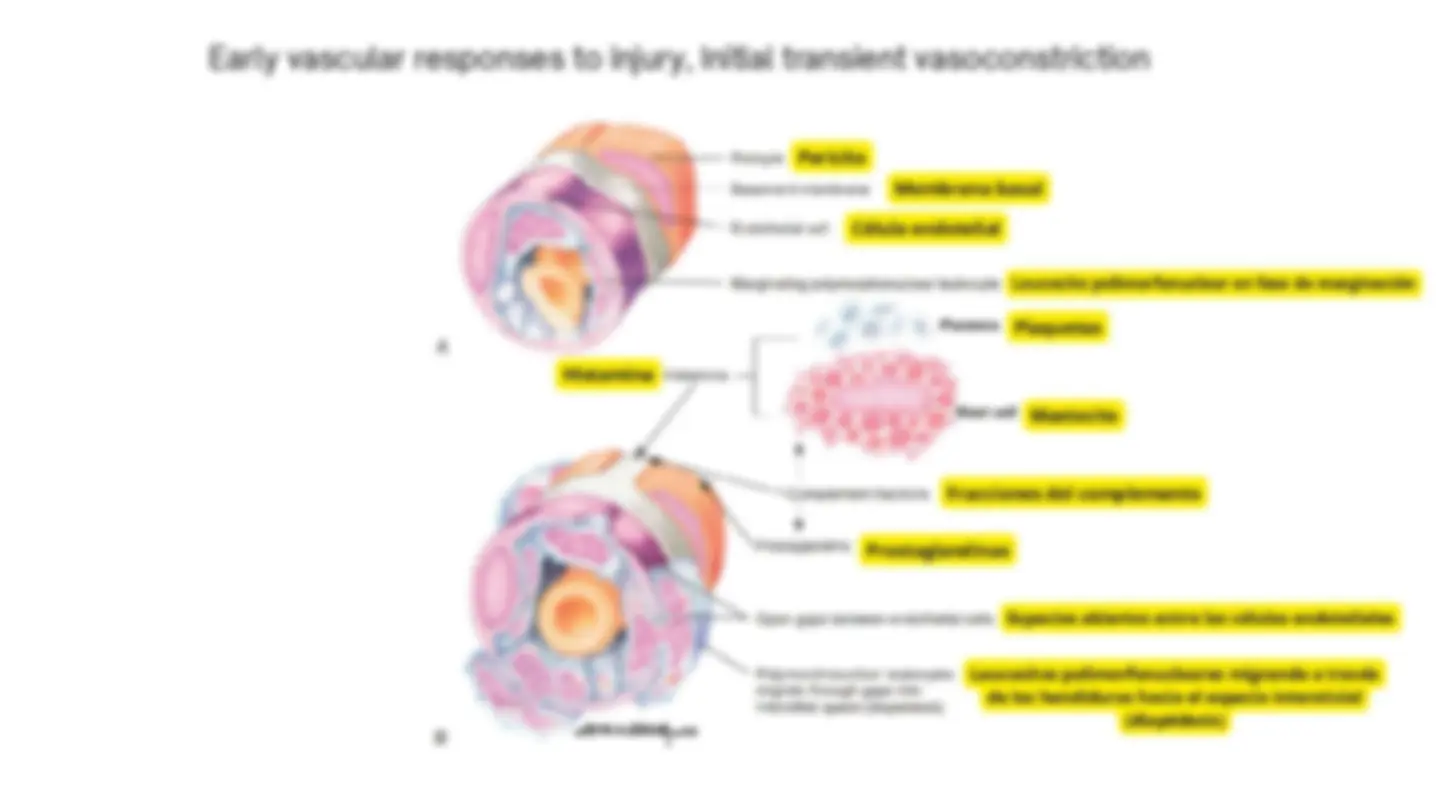
Inflammatory Stage Begins the moment tissue injury occurs and, in the absence of factors that prolong inflammation, lasts 3 to 5 days. The inflammatory stage has 2 phases: Vascular Cellular The vascular events set in motion during inflammation begin with an initial vasoconstriction of disrupted vessels as a result of normal vascular tone. Within minutes, histamine and prostaglandins E1 and E2, elaborated by white blood cells, cause vasodilation and open small spaces between endothelial cells, which allows plasma leak leukocytes to migrate into interstitial tissues. The cellular phase of inflammation is triggered by the activation of serum complement by tissue trauma. Complement-split products, particularly C3a and C5a, act as chemotactic factors and cause polymorphonuclear leukocytes (neutrophils) to stick to the side of blood vessels (margination) and then migrate through the vessel walls (diapedesis).
Fibroplastic Stage The strands of fibrin, which are derived from blood coagulation, crisscross wounds forming a latticework on which fibroblasts begin laying down ground substance and tropocollagen. This is the fibroplastic stage of wound repair. The ground substance consists of several mucopolysaccharides, which act to cement collagen fibers together. The fibroblasts transform local and circulating pluripotential mesenchymal cells that begin tropocollagen production on the third or fourth day after tissue injury
Fibroplastic Stage Fibroblasts deposit tropocollagen, which undergoes cross-linking to produce collagen. Initially, collagen is produced in excessive amounts and is laid down in a haphazard manner. Wound strength rapidly increases during the fibroplastic stage, which normally lasts 2 to 3 weeks. If a wound is placed under tension at the beginning of fibroplasia, it tends to pull apart along the initial line of injury. The poor orientation of fibers decreases the effectiveness of a given amount of collagen to produce wound strength, so an overabundance of collagen is necessary to strengthen the healing wound early on.
Remodeling Stage A final process, which begins near the end of fibroplasia and continues during the early portion of remodeling, is wound contraction. During wound contraction, the edges of a wound migrate toward each other. In a wound in which the edges are not or will not be placed in apposition, wound contraction diminishes the size of the wound. Contraction can be lessened by placement of a layer of epithelium between the free edges of a wound. The surgeon’s goal with respect to scar formation is not to prevent a scar but rather to produce a scar that minimizes any compromise of function and looks as inconspicuous as possible. “ ”
Factors That Impair Wound Healing
Foreign Material Foreign material is everything the host organism’s immune system views as “non-self,” including bacteria, dirt, and suture material. Foreign materials cause three basic problems: First, bacteria can proliferate and cause an infection in which released bacterial proteins destroy host tissue. Second, nonbacterial foreign material acts as a haven for bacteria by sheltering them from host defenses and thus promoting infection. Third, foreign material is often antigenic and can stimulate a chronic inflammatory reaction that decreases fibroplasia.
Necrotic Tissue Necrotic tissue in a wound causes two problems: First, is that its presence serves as a barrier to the ingrowth of reparative cells. The inflammatory stage is then prolonged while white blood cells work to remove the necrotic debris through the processes of enzymatic lysis and phagocytosis. Second, is that, similar to foreign material, necrotic tissue serves as a protected niche for bacteria. Necrotic tissue frequently includes blood that collects in a wound (hematoma), where it can serve as an excellent nutrient source for bacteria.
Ischemia Ischemia can be caused by several things: T ight or incorrectly located sutures I mproperly designed flaps E xcessive external pressure on a wound I nternal pressure on a wound (seen, such as with hematomas) S ystemic hypotension P eripheral vascular disease A nemia
Tension Tension on a wound is the final factor that can impede wound healing. Tension in this case is anything tending to hold wound edges apart. If sutures are used to pull tissues together forcefully, the fine blood vessels in the tissue encompassed by the sutures will be constricted, producing ischemia. If sutures are removed too early in the healing process, the wound under tension will probably reopen and then heal with excessive scar formation and wound contraction. If sutures are left in too long in an attempt to overcome wound tension, the wound will still tend to spread open during the remodeling stage of healing, and the tract into the epithelium through which the sutures ran will epithelialize, leaving permanent, disfiguring marks.